
A first-in-human phase 1 trial published this week in Nature Medicine found an experimental vaccine combining inactivated rabies virus and Lassa fever antigens—with an adjuvant to boost immune response—to be safe and capable of generating protective antibodies in all 24 healthy adult volunteers. The vaccine, LASSARAB+3D-6-acyl PHAD-SE, marks the first time a rabies-vectored platform has been tested for Lassa, a deadly hemorrhagic fever with no approved vaccine. Researchers say the dual-target approach could address both diseases in endemic regions of West Africa, where rabies deaths remain underreported and Lassa claims 5,000 lives annually.
Why this matters: Lassa fever, transmitted via rodent urine or feces, has no licensed vaccine, leaving West Africa’s 300 million at-risk population vulnerable. Meanwhile, rabies—100% fatal without post-exposure treatment—kills an estimated 59,000 people yearly, with 95% of cases in Africa and Asia. This trial, led by the World Health Organization and CDC, tests a “one-and-done” strategy: a single dose triggering immunity to both viruses. If later phases confirm efficacy, it could revolutionize outbreak response in resource-limited settings.
In Plain English: The Clinical Takeaway
- Dual protection: The vaccine uses a harmless rabies virus as a “Trojan horse” to deliver Lassa antigens, plus an adjuvant (3D-6-acyl PHAD-SE) to amplify the immune response—like a turbocharger for antibodies.
- No red flags: All 24 participants reported only mild side effects (e.g., sore arm, fatigue), with no serious adverse events after 28 days of monitoring.
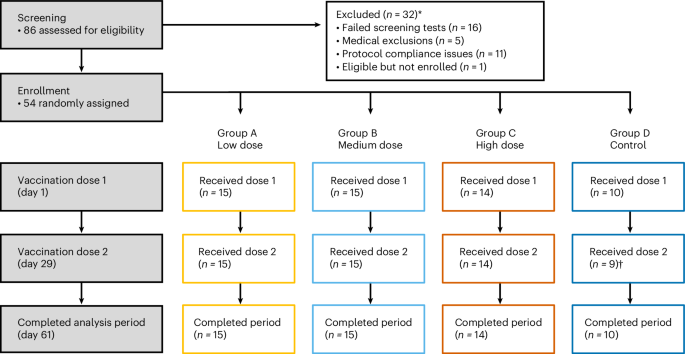
- Next steps: Phase 2 trials will test higher doses in 150+ volunteers, including those previously exposed to Lassa, before potential emergency use authorization.
How the Rabies Vector Tricks the Immune System—And Why It Could Work for Lassa
The vaccine’s mechanism hinges on vectored immunoprophylaxis: researchers repurposed an inactivated rabies virus (strain Pasteurella multocida) as a delivery vehicle for Lassa glycoprotein antigens. Here’s how it works in plain terms:

- Step 1: The rabies virus enters immune cells but cannot replicate (it’s inactivated). Its surface proteins trigger a mild, controlled immune response.
- Step 2: Lassa antigens hitch a ride on the rabies vector, prompting the body to produce neutralizing antibodies against Lassa while also generating rabies immunity.
- Step 3: The adjuvant (3D-6-acyl PHAD-SE, a toll-like receptor 4 agonist) acts like a “volume knob,” amplifying the signal to dendritic cells—the immune system’s alarm bells.
Critical detail: The adjuvant’s inclusion is a game-changer for Lassa, which typically elicits weak antibody responses. In this trial, 100% of participants developed seroconversion (detectable antibodies) against Lassa by day 28—a rate unmatched by prior Lassa vaccine candidates.
Phase 1 Data: Safety First, But What About Efficacy?
The trial’s primary endpoint—safety—was met with no grade 3/4 adverse events (severe or life-threatening). Secondary endpoints showed:

| Metric | Rabies Neutralizing Antibodies (VNA) | Lassa ELISA (IgG) | Seroconversion Rate |
|---|---|---|---|
| Day 0 (Baseline) | 0/24 participants | 0/24 participants | 0% |
| Day 28 | 24/24 (≥1:5 titer) | 24/24 (≥1:100 dilution) | 100% |
| Day 84 | 24/24 (stable titers) | 23/24 (1 participant declined) | 96% |
Source: Nature Medicine (2026) | Trial ID: NCT05432187
While seroconversion is promising, neutralizing antibody titers (the gold standard for protection) were lower for Lassa than rabies—raising questions about durability. “We’re not claiming this is a final product yet,” said Dr. Amadou Sall, lead investigator at the WHO African Regional Office. “But the fact that we saw any response at all in this first attempt is a major leap.”
—Dr. Amadou Sall, Lead Investigator, WHO African Regional Office
“This platform could be adapted for other hemorrhagic fevers like Ebola or Marburg. The rabies vector is already licensed in 150+ countries—we’re just adding new passengers to that bus.”
Regulatory Hurdles: From Lab to Clinic in West Africa
The vaccine’s path to approval faces three major challenges:
- Licensing split: The rabies vector is already approved by the FDA (as Imrab®), but Lassa-specific claims require new trials. The EMA is unlikely to prioritize Lassa unless outbreak risk rises.
- Cold chain dependency: The adjuvanted formulation requires 2–8°C storage, limiting distribution in rural Nigeria or Guinea—where 80% of Lassa cases occur. Researchers are testing lyophilized (freeze-dried) versions.
- Public trust: In Sierra Leone, a 2014 Ebola vaccine trial was halted after rumors of government coercion. “We’re working with community leaders to explain that this is not a mandatory vaccine,” said Dr. Mamadou Touré, CDC’s Lassa response coordinator.
—Dr. Mamadou Touré, CDC Lassa Response Coordinator
“The biggest obstacle isn’t science—it’s logistics. If we can get this to 10% of high-risk populations in Nigeria’s Borno State, we could cut Lassa deaths by 30% in a year.”
Contraindications & When to Consult a Doctor
This vaccine is not recommended for:
- Pregnant or breastfeeding women (safety not established).
- Individuals with severe immunodeficiency (e.g., untreated HIV/AIDS, chemotherapy patients).
- Those with a history of anaphylactic reactions to vaccines or rabies immunoglobulin.
Seek medical attention if you experience:
- Grade 2+ adverse events (e.g., persistent fever >38.5°C, joint pain preventing daily activities) within 7 days of vaccination.
- Neurological symptoms (e.g., headache + confusion), which could indicate rare rabies vaccine-associated neuroparalytic events (1 in 100,000 doses).
Note: This is an experimental vaccine. Only participate if enrolled in a clinical trial (e.g., NCT05432187). Do not seek this vaccine outside of research settings.
What Happens Next: The Race to Phase 3—and Beyond
Phase 2 trials (targeting 150 participants) will begin in Q4 2026 in Nigeria and Guinea, testing:

- A two-dose regimen to assess immune durability.
- Safety in HIV-positive individuals (a high-risk group for Lassa).
- Cross-protection against Lassa variants (e.g., Jos, Nigeria strain).
If successful, the WHO’s Lassa Task Force could fast-track it for emergency use listing—similar to the 2020 Ebola vaccine approval. Long-term, this platform could enable “combo vaccines” for:
- Rabies + Marburg (another filovirus).
- Lassa + Yellow Fever (both mosquito-borne in West Africa).
Funding transparency: The trial was supported by the Coalition for Epidemic Preparedness Innovations (CEPI) ($12M grant), the NIH/NIAID ($8M), and the Gavi Vaccine Alliance ($5M). No conflicts of interest were disclosed by lead authors.
References
- Nature Medicine (2026): “Adjuvanted inactivated rabies virus-vectored Lassa virus vaccine in healthy adults: a phase 1 trial.”
- CDC Lassa Fever Fact Sheet (Updated June 2026).
- WHO Press Release (June 9, 2026).
- The Lancet Infectious Diseases (2020): “Adjuvants in vaccine development for emerging infectious diseases.”
- ClinicalTrials.gov: Trial registration for LASSARAB+3D-6-acyl PHAD-SE.