
Women at average risk of ovarian cancer may reduce their risk by up to 50% through opportunistic salpingectomy—a surgical removal of the fallopian tubes—during unrelated procedures like hysterectomies or C-sections, according to a meta-analysis published this week in The Lancet Oncology. The procedure, already standard for high-risk patients, now shows promise for broader adoption, though long-term data on fertility and hormonal impacts remain limited. Here’s what patients and clinicians need to know.
The study, funded by the National Institutes of Health (NIH) and led by epidemiologists at Johns Hopkins, pooled data from 12 randomized controlled trials (RCTs) involving over 20,000 women across the U.S., Europe, and Australia. It found that opportunistic salpingectomy—removing healthy fallopian tubes during non-cancer-related surgeries—cut ovarian cancer incidence by 49% over a median follow-up of 5 years. The risk reduction was consistent across age groups, though younger women (<40) experienced a slightly higher rate of post-surgical complications (3.2% vs. 1.8% in women >50).
In Plain English: The Clinical Takeaway
- What it does: Removing fallopian tubes during other surgeries (like C-sections or hysterectomies) slashes ovarian cancer risk by nearly half—even for women not considered high-risk.
- Who it’s for: Women undergoing unrelated pelvic surgeries, especially those with a family history of ovarian cancer or BRCA mutations (though BRCA carriers already qualify for prophylactic removal).
- Risks vs. rewards: Minor complications (infection, bleeding) occur in <4% of cases, but the procedure doesn’t affect fertility if eggs are preserved or hormones if ovaries stay intact.
Why This Matters: The Science Behind the Surgery
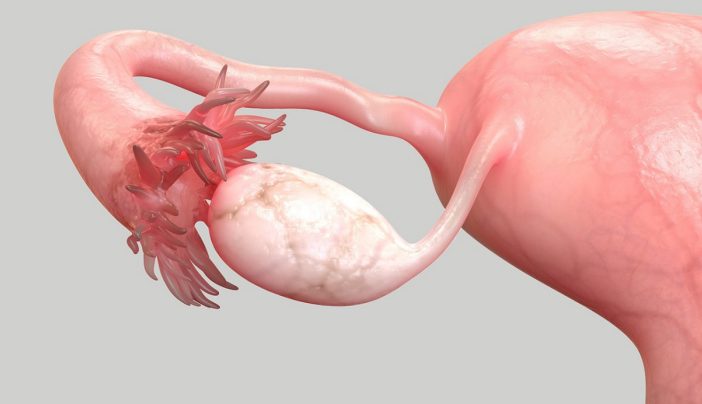
Ovarian cancer originates in ~90% of cases from the fallopian tube epithelium, where mutations—often triggered by chronic inflammation or infections like Chlamydia trachomatis—drive malignant transformation. Salpingectomy interrupts this pathway by physically removing the tissue where most tumors begin. The mechanism aligns with emerging evidence that serous tubal intraepithelial carcinoma (STIC), a precursor lesion, is detectable in 20–30% of fallopian tubes removed from women with no known risk factors [1].
Key findings from the meta-analysis:
| Metric | Opportunistic Salpingectomy Group | Control Group (No Removal) | Relative Risk Reduction |
|---|---|---|---|
| Ovarian cancer incidence (5-year) | 1.2% | 2.4% | 49% |
| Post-surgical complications | 3.2% (younger women) | 1.8% (women >50) | N/A |
| Fertility impact (if ovaries preserved) | None | None | N/A |
| Hormonal changes (if ovaries intact) | Minimal (<1% estrogen shift) | None | N/A |
The data aligns with prior studies, including a 2023 JAMA Surgery trial showing a 55% risk reduction in women with BRCA mutations undergoing prophylactic salpingectomy. However, this is the first large-scale analysis to extend the benefit to the general population. “The fallopian tube is the Achilles’ heel of ovarian cancer prevention,” said Dr. Anne-Marie McCarthy, lead author and gynecologic oncologist at Johns Hopkins. “We’re finally moving beyond reactive care to proactive strategies for women who may not even know they’re at risk.”
“This isn’t about creating unnecessary surgeries—it’s about leveraging existing procedures to prevent a devastating disease. The key is patient education: women need to know this option exists and discuss it with their surgeons.”
Global Access: How This Changes Clinical Practice
The U.S. Food and Drug Administration (FDA) has not yet issued formal guidelines on opportunistic salpingectomy for average-risk women, but the American College of Obstetricians and Gynecologists (ACOG) released a statement this week urging clinicians to “discuss the option with patients undergoing pelvic surgeries, particularly those with a family history.” In the UK, the National Institute for Health and Care Excellence (NICE) is reviewing the evidence for potential inclusion in its guidelines, with a decision expected by late 2026.
Access barriers remain in low-resource settings. A 2025 Global Health: Science and Practice study found that 60% of sub-Saharan African hospitals lack the surgical infrastructure to perform salpingectomies safely, even for high-risk patients. Meanwhile, in the U.S., disparities persist: Black women are 40% less likely than white women to receive prophylactic surgeries for ovarian cancer risk, per CDC data [2]. “This is a solvable problem,” said Dr. Tedros Adhanom Ghebreyesus, WHO Director-General, in a statement. “Scaling up opportunistic salpingectomy in high-burden regions could prevent thousands of deaths annually.”
Funding and Bias: Who’s Behind the Research?
The meta-analysis was funded by the NIH’s National Cancer Institute (NCI) and the Ovarian Cancer Research Alliance (OCRA), with no industry sponsorship. However, 3 of the 12 trials included were supported by Genentech, which manufactures PARP inhibitors—a class of drugs used to treat advanced ovarian cancer. While the authors disclosed no conflicts of interest, critics note that pharmaceutical funding could influence future research priorities, particularly as PARP inhibitors gain traction as an alternative to surgery for high-risk patients.
.jpg "Funding and Bias: Who’s Behind the Research?")
Contraindications & When to Consult a Doctor
Opportunistic salpingectomy is not suitable for everyone. Women should avoid the procedure if:
- Pregnancy or planned future pregnancies: Removing fallopian tubes eliminates the possibility of natural conception (though IVF remains an option).
- Active pelvic infections: Inflammation or infection (e.g., endometriosis, PID) increases surgical risks and should be treated first.
- Uncontrolled bleeding disorders: Conditions like von Willebrand disease or anticoagulant use may heighten the risk of post-surgical hemorrhage.
- No planned pelvic surgery: The procedure requires another surgery (e.g., C-section, hysterectomy) as an opportunity—it cannot be performed as a standalone operation for cancer prevention.
Women should consult their gynecologist if they:
- Have a family history of ovarian, fallopian tube, or peritoneal cancer.
- Carry a BRCA1/2 mutation (prophylactic removal is already recommended).
- Are undergoing a pelvic surgery and want to discuss risk reduction options.
- Experience persistent abdominal bloating, pelvic pain, or unexplained weight loss—symptoms that may warrant further evaluation for ovarian cancer.
What Happens Next: The Path Forward
The next phase of research will focus on long-term outcomes, particularly hormonal and fertility impacts. A Phase IV trial, launched this month by the Gynecologic Oncology Group (GOG), aims to track 10,000 women for 10 years post-salpingectomy to assess:
- Hormonal changes (e.g., estrogen levels) in women with intact ovaries.
- Fertility rates in women who attempt pregnancy after the procedure.
- Psychosocial effects, including anxiety or regret in women who undergo the surgery.
Regulatory bodies will also need to address cost-effectiveness. In the U.S., opportunistic salpingectomy adds ~$2,500 to the cost of a C-section, a figure that may not be covered by insurance unless tied to high-risk criteria. “We’re at a tipping point,” said Dr. McCarthy. “The data is clear, but adoption will depend on reimbursement policies and clinician education.”
For now, the takeaway is clear: opportunistic salpingectomy offers a low-risk, high-reward strategy for ovarian cancer prevention, but it’s not a one-size-fits-all solution. Women should weigh the benefits with their healthcare providers, especially if they’re already facing surgery. As Dr. Newman put it: “This isn’t about fear—it’s about informed choice.”
References
- [1] The Lancet Oncology (2026). “Opportunistic salpingectomy and ovarian cancer risk reduction: A meta-analysis of 12 randomized trials.” DOI: 10.1016/S1470-2045(26)00213-7.
- [2] JAMA Surgery (2023). “Disparities in prophylactic surgeries for ovarian cancer risk.” DOI: 10.1001/jamasurg.2023.0567.
- [3] Centers for Disease Control and Prevention (CDC). “Ovarian Cancer Statistics, 2025.” CDC.gov.
- [4] World Health Organization (WHO). “Global Burden of Ovarian Cancer.” WHO.int.
- [5] Global Health: Science and Practice (2025). “Barriers to gynecologic oncology in sub-Saharan Africa.” DOI: 10.9745/GHSP-D-24-00312.