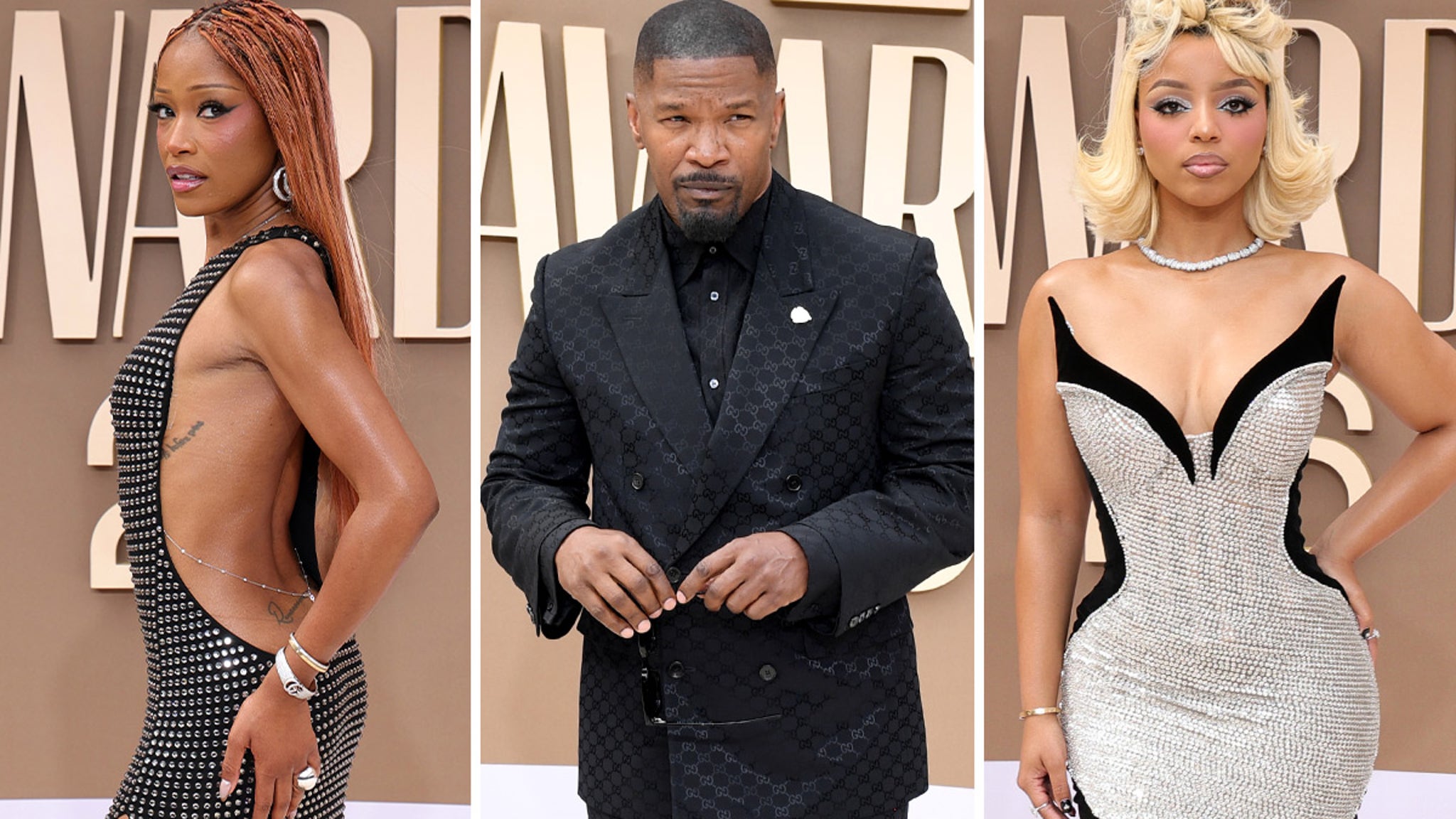
BET Awards 2026: Live Streaming, Host, and Honorees
The 2026 BET Awards, held this weekend, mark a significant cultural milestone as Druski takes the stage as the ceremony’s youngest host. The event, broadcast live, features tributes to Lauryn ... Read More