

SEGA Announces New Sonic Short: Memories and Beyond
SEGA announced the upcoming animated short Sonic the Hedgehog: Memories and Beyond during Anime Expo 2026. The film is scheduled for release in late 2026 to coincide with the 35th ... Read More
Saturday Edition
Stay updated with Archyde – your source for breaking news, global headlines, economy, entertainment, health, technology, and sports. Fresh stories daily.
SEGA announced the upcoming animated short Sonic the Hedgehog: Memories and Beyond during Anime Expo 2026. The film is scheduled for release in late 2026 to coincide with the 35th ... Read More
Continuous Coverage

Animaccord, the studio behind the global hit Masha and the Bear, has officially refuted allegations characterizing the animated…

China is moving to overhaul its Electronic Commerce Law to tighten oversight of digital platforms and data-intensive corporations.…

Mourners gathered in Tehran for the funeral of President Ebrahim Raisi, who died in a helicopter crash in…

Savannah James and April McDaniel have launched Signed, a new holding company designed to scale women-focused brands and…
Michael Platt, co-founder of BlueCrest Capital Management, faced a protracted dispute with HM Revenue & Customs (HMRC) over…
California Maintains Transgender Sports Policy Despite SCOTUS Ruling California Governor Gavin Newsom’s administration has confirmed that state policies…
Global Affairs

Morocco won a viral social media “food battle” against Canada this week, with Moroccan staples like Tajine and…
Markets And Money

Spain currently hosts 56,682 electric vehicle (EV) charging points, yet approximately a quarter of this infrastructure remains non-operational,…
Digital Culture

The U.S. Department of Transportation has proposed a regulatory shift to replace the 53-year-old ban on civilian supersonic…
Science And Wellbeing
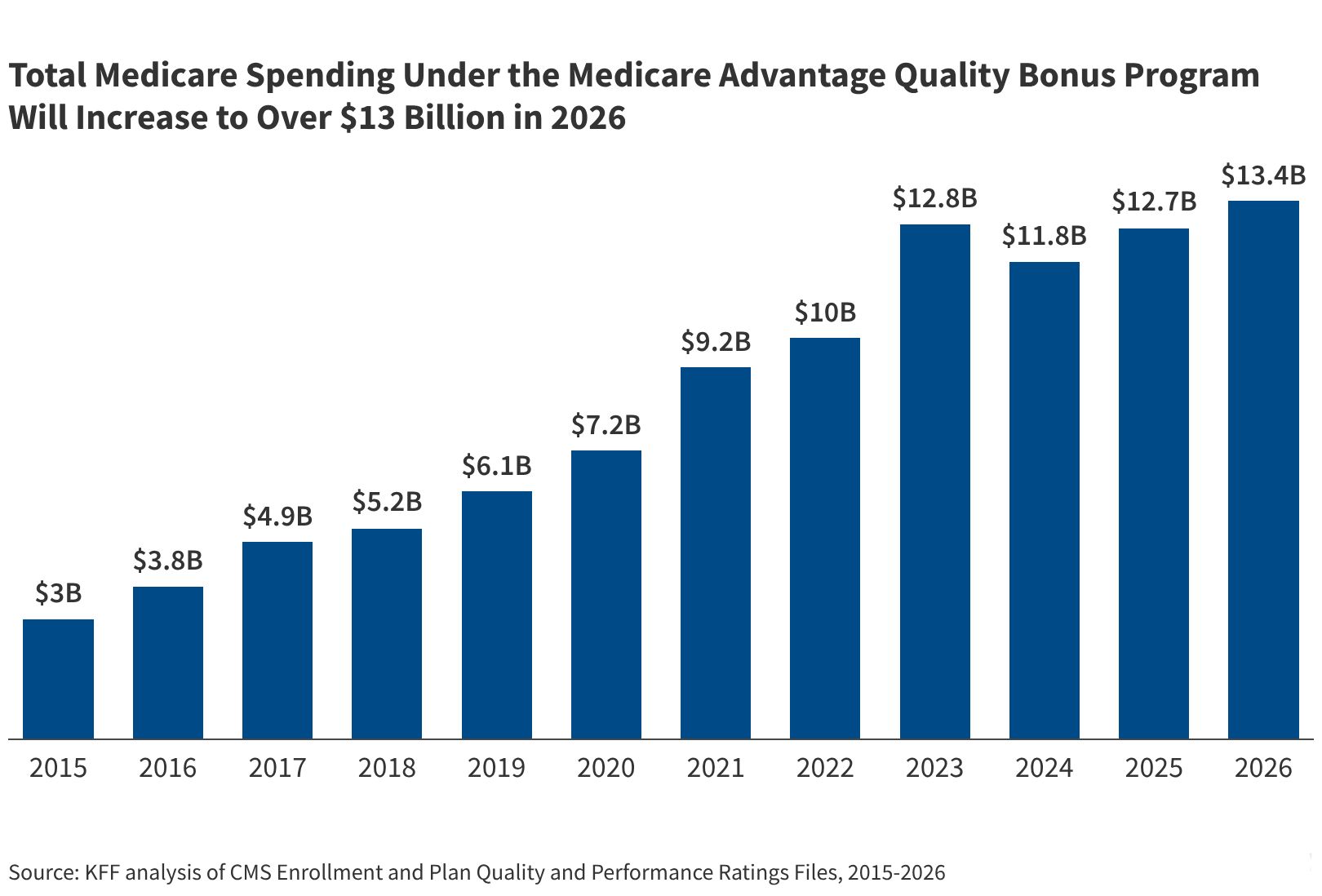
The Medicare program will spend at least $13 billion on the Medicare Advantage quality bonus program in 2026.…
Screen And Sound

Kazuo Ishiguro’s recent reflection on train-set films, published in The Times on July 4, 2026, highlights how confined…
Fixtures And Form

Who, What, Where, Why: The 2026 Tour de France Bike Selection Sparks Debate Over Performance and Value The…


