

Xiaomi 17T Pro Campaign Price: 58,280 TL
Xiaomi has discounted the 512 GB model of the Xiaomi 17T Pro to 58,280 TL in Turkey as of July 3, 2026. The device features the MediaTek Dimensity 9500 chipset, ... Read More
Saturday Edition
Stay updated with Archyde – your source for breaking news, global headlines, economy, entertainment, health, technology, and sports. Fresh stories daily.
Xiaomi has discounted the 512 GB model of the Xiaomi 17T Pro to 58,280 TL in Turkey as of July 3, 2026. The device features the MediaTek Dimensity 9500 chipset, ... Read More
Continuous Coverage

Chanel’s Masculine Pivot: Decoding the Brand’s Strategic Shift Toward Men’s Ready-to-Wear Chanel is increasingly leveraging high-profile male ambassadors,…

Bitcoin (BTC) surpassed $61,000 as weaker-than-expected U.S. employment data increased market expectations for Federal Reserve interest rate cuts.…

NATO leaders, including Trump, are gathering in Ankara this week to formalize an “ironclad commitment” to collective defense,…

A 25-question superquiz designed to test readers’ knowledge has been launched by world-today-news.com, according to a published image.…

Two Romanian nationals were sentenced in London on July 3, 2026, for orchestrating an attack on opposition journalist…

A 27-year-old woman has denied allegations of a consensual encounter in a rape trial involving Michael Ward, a…
Global Affairs
The second edition of Brazil DNA, held Friday in São Paulo, connected Brazilian tourism operators and destinations with…
Markets And Money

Morocco has imposed anti-dumping duties on steel sheets imported from Egypt to protect its domestic metallurgical industry from…
Digital Culture

Android 17, currently deploying to Pixel devices, introduces three settings hidden within the menus that change how the…
Science And Wellbeing

Recent computational simulations have identified that alpha particles—previously viewed as a potential hindrance in fusion reactors—may actually stabilize…
Screen And Sound

As temperatures in Benalmádena soar this July 2026, families are increasingly turning to climate-controlled indoor entertainment and off-peak…
Fixtures And Form
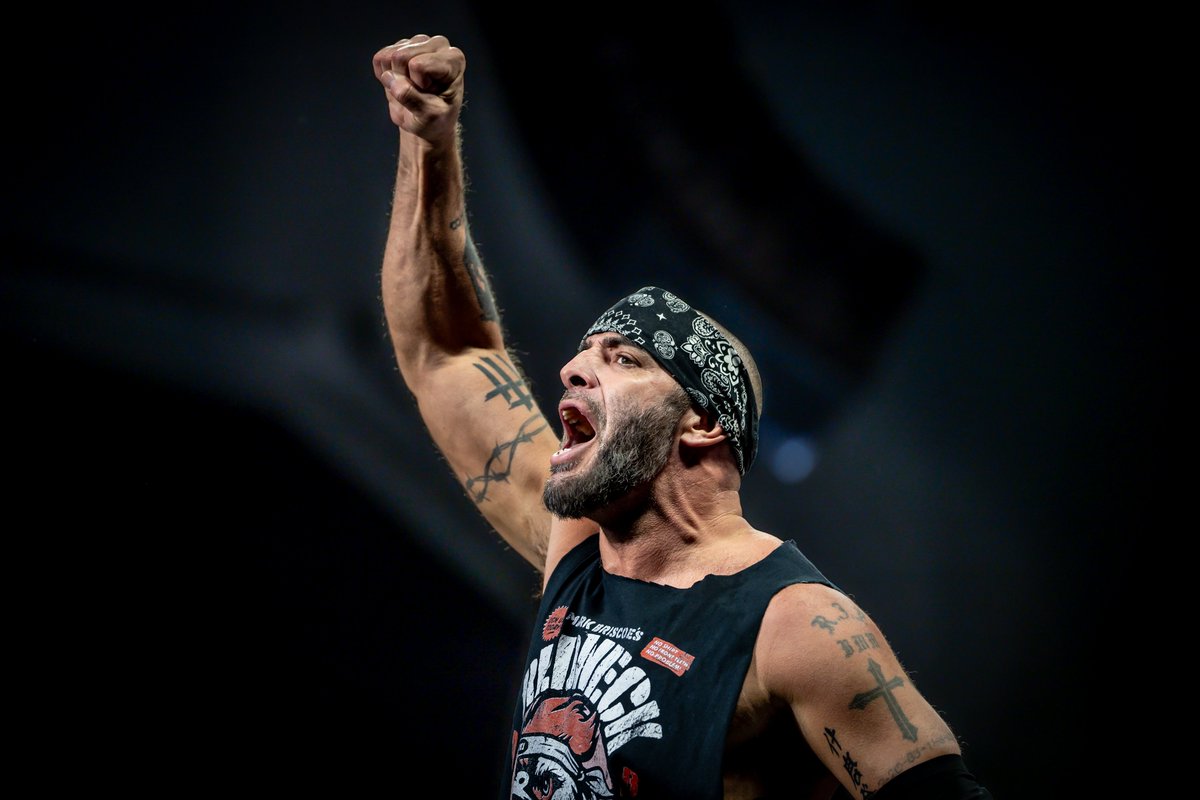
AEW star Mark Briscoe is sidelined with a legitimate injury following a World Championship match against MJF on…

