
Mexico Faces Title Favorites in Round of 16
Mexico faces England in the Round of 16 of the 2026 FIFA World Cup on July 5, 2026. As one of the three host nations, Mexico’s “El Tri” seeks to ... Read More

Saturday Edition
Stay updated with Archyde – your source for breaking news, global headlines, economy, entertainment, health, technology, and sports. Fresh stories daily.
Mexico faces England in the Round of 16 of the 2026 FIFA World Cup on July 5, 2026. As one of the three host nations, Mexico’s “El Tri” seeks to ... Read More
Continuous Coverage
The rise of digital subcultures on platforms like DC Inside has created a volatile ecosystem for South Korean…

Benin’s Minister of Economy and Finance, Romuald Wadagni, is currently abroad as of July 5, 2026, on an…

The Australian government is pivoting from consumer-facing AI chatbots toward “GovStack” infrastructure—a modular, backend digital architecture designed to…
Egypt Expands Scope of Ninth Cairo Water Week to Address Global Water Security Egypt is expanding the international…

Noah Wyle Missed Oscar Role Due to ‘ER’ Commitments, Industry Implications Explored When Noah Wyle couldn’t escape ‘ER’…

Seattle’s emergence as a premier soccer hub is driving a measurable shift in community health, as longitudinal data…
Global Affairs
As of July 5, 2026, the United Kingdom’s mid-tier finance recruitment market is signaling a tightening demand for…
Markets And Money

Saint-Ciers-sur-Gironde has transformed the Georges-Brassens school courtyard into a “green yard,” replacing asphalt with permeable surfaces and vegetation.…
Digital Culture

ZenaTech is upgrading its IQ Nano indoor drone platform with enhanced visual processing and expanded data automation capabilities…
Science And Wellbeing

The World Health Organization (WHO) officially declared the end of the hantavirus episode this July, confirming that the…
Screen And Sound
Multiple heat-related illnesses at July 4 events on the National Mall spark scrutiny of public event safety protocols,…
Fixtures And Form
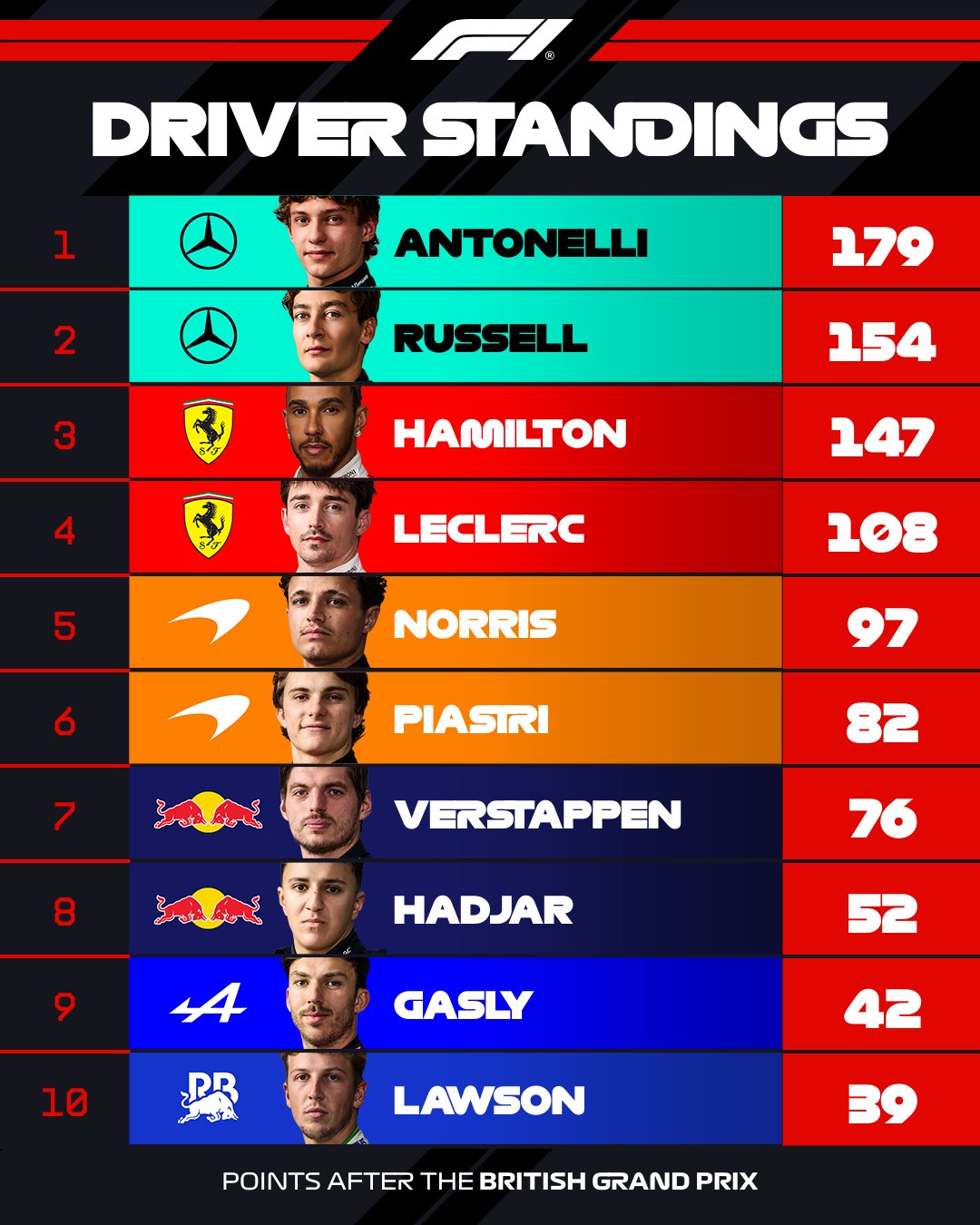
After nine rounds of the 2026 Formula 1 season, Luca Antonelli’s 25-point lead in the Drivers’ Championship has…



