
{kind=link}
Rare Adalimumab Reaction Mimics Methotrexate Side Effect, Challenging Diagnosis
Table of Contents
- 1. Rare Adalimumab Reaction Mimics Methotrexate Side Effect, Challenging Diagnosis
- 2. What are the key immunological mechanisms by which adalimumab increases the risk of *Pneumocystis jirovecii* pneumonia?
- 3. Adalimumab-Induced Pneumocystis jirovecii Pneumonitis: A Diagnostic Challenge
- 4. Understanding the Link Between TNF-α inhibitors and Pneumocystis Pneumonia
- 5. Why Adalimumab Increases PCP Risk
- 6. Clinical Presentation: Atypical Symptoms & Diagnostic Delays
- 7. Diagnostic Tools & Techniques
- 8. Prophylaxis & Prevention Strategies
A recent case underscores the critical need for differential diagnosis when patients on Adalimumab present with respiratory symptoms.
A perplexing medical scenario has surfaced, illustrating the intricate challenges in diagnosing lung conditions in patients undergoing treatment for autoimmune diseases. A case report detailed how a patient,
What are the key immunological mechanisms by which adalimumab increases the risk of *Pneumocystis jirovecii* pneumonia?
Adalimumab-Induced Pneumocystis jirovecii Pneumonitis: A Diagnostic Challenge
Understanding the Link Between TNF-α inhibitors and Pneumocystis Pneumonia
Pneumocystis jirovecii pneumonia (PCP), a fungal infection primarily affecting individuals with weakened immune systems, is increasingly recognized as a potential complication in patients treated with tumor necrosis factor-alpha (TNF-α) inhibitors like adalimumab (Humira). While traditionally associated with HIV/AIDS, the rising use of biologic therapies for autoimmune conditions – rheumatoid arthritis, Crohn’s disease, ulcerative colitis, psoriasis – has led to a resurgence of PCP, often presenting diagnostic hurdles. This article explores the complexities of adalimumab-induced PCP, focusing on risk factors, diagnostic approaches, and preventative strategies.
Why Adalimumab Increases PCP Risk
Adalimumab, a TNF-α blocker, suppresses the immune system by neutralizing TNF-α, a key cytokine involved in inflammation.While effective in managing autoimmune diseases, this immunosuppression can compromise the host’s defense against opportunistic infections like P. jirovecii.
Here’s how adalimumab contributes to increased risk:
impaired Cell-Mediated Immunity: TNF-α is crucial for activating macrophages and T-cells, essential components of the immune response against Pneumocystis.
Reduced Inflammatory Response: While the goal of adalimumab is to reduce inflammation, a certain level of inflammation is necessary for effective immune function.
Co-morbidities & Concomitant Medications: Many patients on adalimumab have underlying conditions or are taking other immunosuppressants (like corticosteroids, methotrexate) further weakening their immune systems.
Clinical Presentation: Atypical Symptoms & Diagnostic Delays
The presentation of adalimumab-associated PCP can be atypical, leading to delays in diagnosis. Symptoms often mimic other respiratory infections, making it arduous to distinguish from common illnesses like influenza or bacterial pneumonia.
Common symptoms include:
Dry Cough: Frequently enough the initial symptom, persistent and non-productive.
Shortness of Breath (Dyspnea): Gradually worsening, even with minimal exertion.
Fever: Might potentially be low-grade or absent, particularly in immunosuppressed individuals.
Fatigue: Important and debilitating.
Hypoxemia: Low blood oxygen levels, detectable through pulse oximetry.
Diagnostic Challenges:
Atypical Radiographic Findings: Chest X-rays may show diffuse interstitial infiltrates, but can also be normal or show subtle changes.
Low Clinical Suspicion: Physicians may not instantly consider PCP in patients on adalimumab presenting with respiratory symptoms.
False-Negative Results: Customary diagnostic tests can have limitations (see below).
Diagnostic Tools & Techniques
Accurate and timely diagnosis is critical for effective treatment. Several diagnostic methods are employed, but each has its strengths and weaknesses.
- Microscopic Examination:
Induced Sputum: The gold standard, but sensitivity can be low (50-80%) due to the small number of organisms present. Multiple samples are recommended.
Bronchoalveolar Lavage (BAL): Offers higher sensitivity (80-95%) but is more invasive. BAL fluid is examined for P. jirovecii cysts using microscopy (Giemsa or Wright-Giemsa stain).
- Polymerase Chain Reaction (PCR): Highly sensitive and specific for detecting P.jirovecii DNA in respiratory samples (sputum, BAL). Increasingly used as a first-line diagnostic test.
- β-D-Glucan Assay: A fungal cell wall component detectable in serum. Can be elevated in PCP, but also in other fungal infections, limiting its specificity. Useful as an adjunct test.
- Chest Imaging:
Chest X-ray: initial imaging modality,but often non-specific.
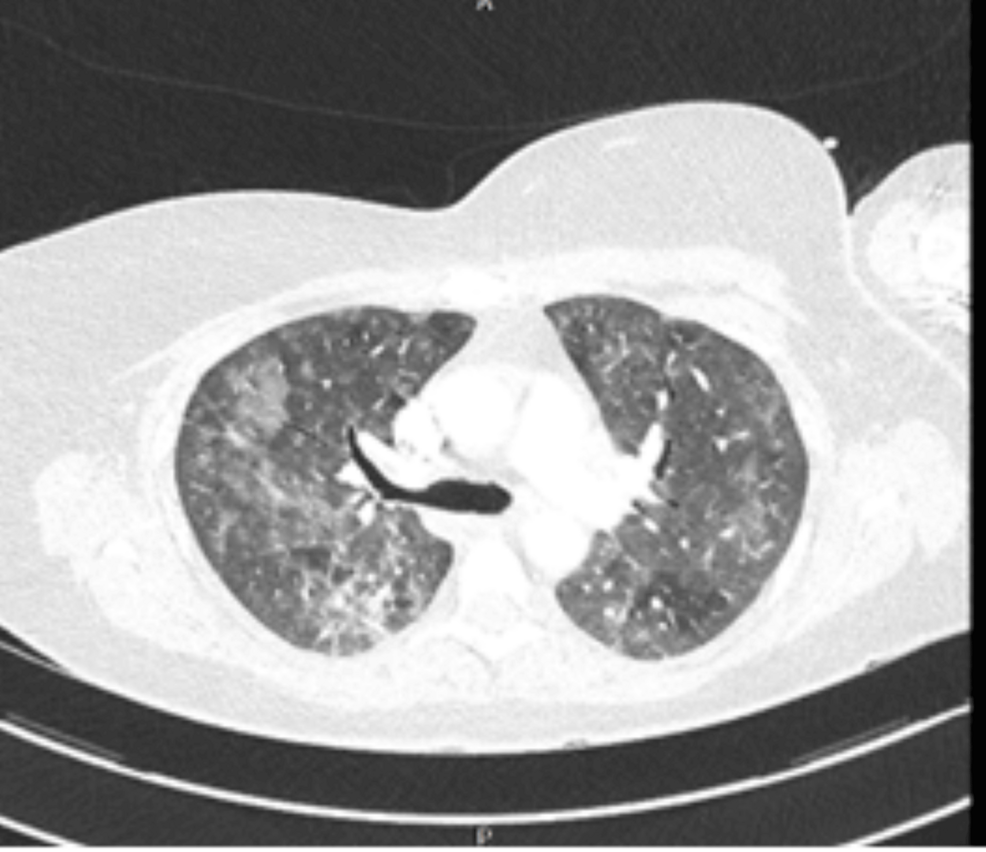
High-resolution Computed Tomography (HRCT): more sensitive for detecting ground-glass opacities and cysts,characteristic of PCP.
Prophylaxis & Prevention Strategies
Preventing PCP in patients on adalimumab is paramount.
Prophylactic Trimethoprim-Sulfamethoxazole (TMP-SMX): The moast commonly used prophylactic agent. Administered daily or weekly, depending on risk stratification.
* Alternative Prophylaxis: For patients intolerant to TMP-