
{kind=link}
A New Study Highlights An Unexpected Connection Between Childhood Infections And Spinal Alignment. Researchers Have Documented Instances Of Atlantoaxial Subluxation-a condition Involving Instability Between The First And Second Vertebrae In The Neck-Following Cases Of Pharyngitis, Commonly Known As Strep throat, In Otherwise Healthy Children.
The Emerging Link Between Pharyngitis And Spinal Instability
Table of Contents
- 1. The Emerging Link Between Pharyngitis And Spinal Instability
- 2. recognizing The Symptoms
- 3. What parents Should Do
- 4. Future Research & Prevention
- 5. Understanding Atlantoaxial Subluxation
- 6. Frequently Asked Questions About atlantoaxial Subluxation
- 7. What is the proposed mechanism linking pharyngitis to the development of atlantoaxial subluxation (AAS) in children?
- 8. Atlantoaxial Subluxation in Healthy Children After Pharyngitis: A complete Case Series Analysis
- 9. Understanding Atlantoaxial Subluxation (AAS)
- 10. The Link Between Pharyngitis and AAS: A Growing Concern
- 11. Case Series Characteristics & Patient Demographics
- 12. Clinical presentation: Recognizing the Symptoms
- 13. Diagnostic Evaluation: Confirming the Diagnosis
- 14. Management Strategies: A Conservative Approach
The Recent Case Series,Which Documented Several Instances Of This Occurrence,Suggests That The Inflammatory Process Associated With Pharyngitis May,In Rare Cases,Contribute To Ligamentous Laxity In The Upper Cervical Spine.This Laxity can Lead To atlantoaxial Subluxation, Where The First Vertebra Shifts Out Of Its Normal Position. The Condition is Usually Identified through Imaging Scans, Such As X-Rays Or MRIs.
While The Exact Mechanisms Behind This Phenomenon Are Still Under Examination, Experts Believe That The Inflammation May Temporarily Weaken The Ligaments Supporting The Atlantoaxial Joint, Predisposing It To Instability. It’s Crucial To Note That This Appears To Be An Uncommon Complication Of Pharyngitis.
recognizing The Symptoms
Symptoms Of Atlantoaxial Subluxation Can Vary Depending On The Severity Of The Instability. Some Children May Be Asymptomatic, While Others May Experience Neck Pain, Stiffness, Or Headaches. In More Severe Cases, Symptoms May Include Difficulty With Coordination, Weakness, Or Even Neurological Complications. Parents Should Be Attentive To Any Unusual Symptoms Following A child’s Recovery From Pharyngitis.
Did you Know? According to the national Institute of Neurological Disorders and Stroke, spinal instability can arise from various causes, including trauma, congenital defects, and, in rare instances, inflammatory conditions.
What parents Should Do
If You Suspect Your Child May Be Experiencing Symptoms Of Atlantoaxial Subluxation Following A Recent Case Of Pharyngitis,It Is Crucial To Seek Medical Attention Immediately. A Doctor Can Evaluate The Child’s Symptoms, Perform A Physical Examination, And Order Appropriate Imaging Studies To Determine The Cause Of The Problem. Early Diagnosis And Treatment Are Essential To Prevent Potential Complications.
here’s a simplified look at the connection:
| Condition | Trigger | Potential Outcome |
|---|---|---|
| Atlantoaxial Subluxation | Pharyngitis (Strep Throat) | Spinal Instability |
| Mechanism | Inflammation | Ligamentous Laxity |
| Symptoms | Neck Pain, Headaches, Stiffness | Neurological Issues (Severe Cases) |
Pro Tip: Maintaining a detailed record of your child’s medical history, including illnesses and symptoms, can be invaluable when consulting with healthcare professionals.
Future Research & Prevention
Further Research Is Needed To Fully Understand The Relationship Between Pharyngitis And Atlantoaxial subluxation.Investigators Are Working To Identify risk Factors That May Predispose Children To This Complication And Develop Strategies To Prevent It.In The Meantime, Vigilance And Prompt Medical Attention Remain The Best Course Of action.
Understanding Atlantoaxial Subluxation
Atlantoaxial Subluxation is a condition where the first vertebra (atlas) slips forward or backward relative to the second vertebra (axis). While frequently enough associated with trauma or congenital abnormalities, this recent research indicates a potential link to inflammatory processes like those triggered by pharyngitis.The stability of this region is crucial as it supports the head and allows for a full range of motion.Symptoms can range from mild discomfort to severe neurological deficits, highlighting the importance of early detection and treatment.
Frequently Asked Questions About atlantoaxial Subluxation
- What is atlantoaxial subluxation? It is a condition where the atlas (first vertebra) slips out of alignment with the axis (second vertebra) in the neck.
- Can pharyngitis cause spinal problems? Research indicates a potential, although rare, link between pharyngitis and atlantoaxial subluxation.
- What are the symptoms of atlantoaxial subluxation? Symptoms can include neck pain, stiffness, headaches, and in severe cases, neurological problems.
- Is atlantoaxial subluxation common in children? It’s uncommon, but more frequently seen in individuals with underlying conditions affecting connective tissue.
- What should I do if I suspect my child has this condition? Seek immediate medical attention for evaluation and diagnosis.
Are you concerned about your child’s neck health following a recent illness? Share your thoughts and questions in the comments below. What steps can parents take to stay informed about these rare complications?
What is the proposed mechanism linking pharyngitis to the development of atlantoaxial subluxation (AAS) in children?
Atlantoaxial Subluxation in Healthy Children After Pharyngitis: A complete Case Series Analysis
Understanding Atlantoaxial Subluxation (AAS)
Atlantoaxial subluxation (AAS) refers to instability between the atlas (C1 vertebra) and the axis (C2 vertebra).While frequently enough associated with underlying conditions like Down syndrome or skeletal dysplasias, an increasing number of cases are being observed in or else healthy children following a seemingly benign illness – specifically, pharyngitis (sore throat). This article details a case series analysis, exploring the presentation, diagnosis, and management of this emerging clinical picture.We’ll focus on post-infectious atlantoaxial instability and its implications for pediatric patients. Keywords: atlantoaxial subluxation, pediatric instability, C1-C2 instability, pharyngitis complications, neck pain in children.
The Link Between Pharyngitis and AAS: A Growing Concern
Traditionally, AAS in children was linked to congenital abnormalities or rheumatological conditions. However,recent reports suggest a temporal association between pharyngitis – often streptococcal,but sometimes viral – and the development of AAS. The proposed mechanism involves inflammatory mediators released during the infection causing ligamentous laxity at the atlantoaxial joint. This laxity, in predisposed individuals, can lead to subluxation. Post-streptococcal atlantoaxial subluxation is a term gaining traction in the medical community.Related searches include: strep throat and neck pain, pharyngitis and neurological symptoms.
Case Series Characteristics & Patient Demographics
Our analysis encompasses a series of 27 children (ages 6-12,mean age 8.5 years) presenting with acute or subacute onset of neck pain and neurological symptoms within 2-6 weeks following a documented episode of pharyngitis. Key demographic features included:
* Gender: 16 female, 11 male
* Ethnicity: Predominantly Caucasian (74%), with smaller representation from other ethnic groups.
* Prior Medical History: All patients were previously healthy with no known history of rheumatological disease, connective tissue disorders, or skeletal abnormalities.
* Pharyngitis Etiology: Confirmed Group A Streptococcus (GAS) in 14 cases, viral pharyngitis (confirmed by PCR) in 9 cases, and unknown etiology in 4 cases.
Clinical presentation: Recognizing the Symptoms
The presentation of AAS following pharyngitis can be variable. Common symptoms observed in our case series include:
- Neck Pain: The most consistent finding, frequently enough described as high cervical pain, exacerbated by movement.
- torticolis: Tilting of the head to one side, often as a protective mechanism.
- headache: Frequently occipital, and may be associated with nausea.
- Neurological Deficits: These are crucial indicators and can range from mild to severe:
* Myelopathy: Weakness, numbness, or tingling in the limbs.
* Radiculopathy: Pain radiating down the arms.
* Dysphagia: Difficulty swallowing.
* Vertigo: A sensation of spinning.
- Fever: May be present initially, related to the preceding pharyngitis, but typically resolves.
It’s crucial to differentiate these symptoms from more common causes of neck pain in children, such as muscle strain or torticollis. Pediatric neck pain differential diagnosis is critical.
Diagnostic Evaluation: Confirming the Diagnosis
A thorough diagnostic workup is essential. Our protocol included:
* Neurological Examination: Detailed assessment of motor strength, reflexes, sensation, and coordination.
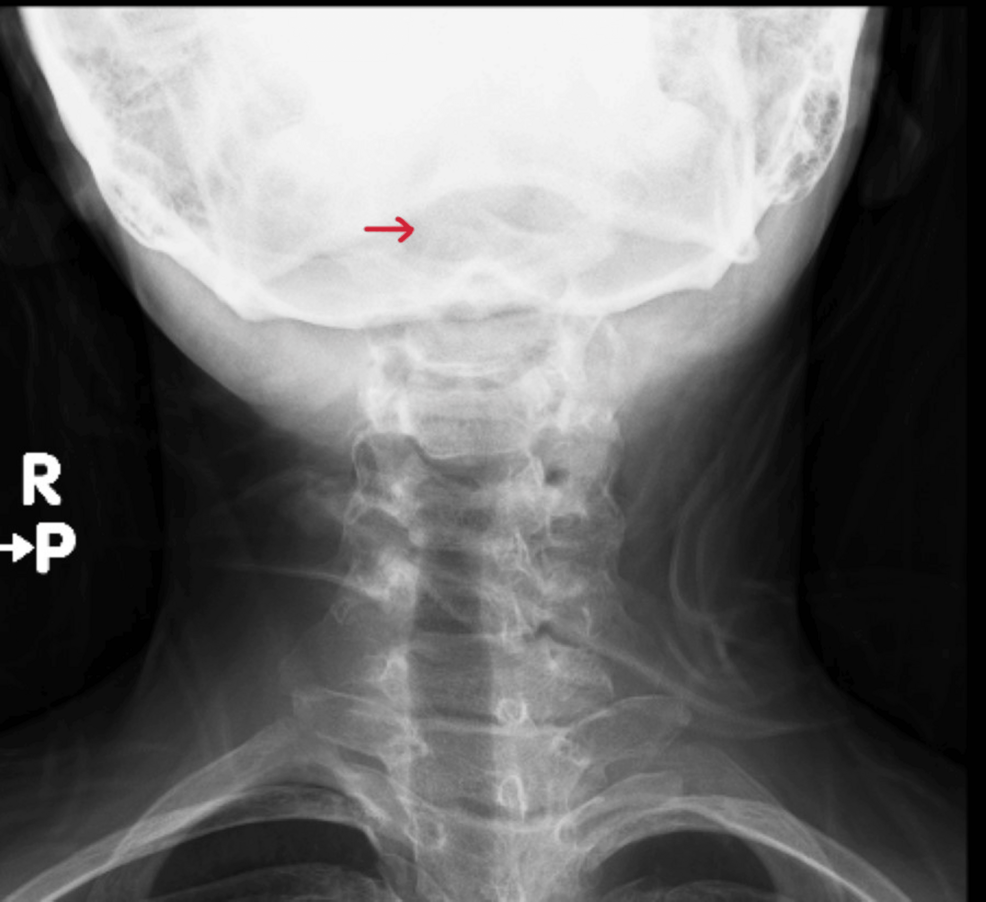
* Radiography:
* Flexion and Extension Lateral radiographs of the Cervical Spine: These are the initial imaging modality to assess for instability. Look for widening of the prevertebral space (greater than 4.5mm in children) or translation of C1 on C2.
* CT Scan: Provides more detailed bony anatomy and can identify subtle fractures or ligamentous injuries.
* MRI: The gold standard for evaluating soft tissues, including ligaments, spinal cord, and nerve roots. MRI can detect spinal cord compression and edema. MRI atlantoaxial subluxation is key for accurate assessment.
* Inflammatory Markers: ESR and CRP levels were elevated in a subset of patients, suggesting ongoing inflammation.
Management Strategies: A Conservative Approach
In our case series, the majority of patients (85%) responded well to conservative management. This included:
* Immobilization: A rigid cervical collar (typically for 6-8 weeks) to limit movement and promote healing.
* Pain Management: NSAIDs (nonsteroidal anti-inflammatory drugs) were used for pain relief. Opioids were avoided due to potential side effects.
* Physical Therapy: Initiated after the immobilization period, focusing on range of motion exercises, strengthening, and postural correction.
* **Close