

Magnesium supplementation, specifically in highly bioavailable forms like magnesium glycinate and malate, supports muscle recovery and bone density by regulating neuromuscular transmission and mineral deposition. These specific chelates are preferred over cheaper oxides due to superior intestinal absorption and reduced gastrointestinal distress in adult populations.
For the average patient, the distinction between different forms of magnesium is not merely a matter of branding, but of biochemistry. While the general public often views “magnesium” as a single entity, the medical community recognizes a spectrum of bioavailability—the proportion of a nutrient that enters the circulation when administered. When we discuss repairing muscles and bones, we are discussing the optimization of the mechanism of action (the specific biochemical process through which a substance produces its effect) regarding ATP production and calcium signaling.
In Plain English: The Clinical Takeaway
- Not all magnesium is equal: Avoid “magnesium oxide” if you seek muscle recovery; it is poorly absorbed and mostly acts as a laxative.
- Targeted Recovery: Magnesium Malate is generally superior for muscle soreness and energy, while Magnesium Glycinate is better for sleep and nerve relaxation.
- Bone Health: Magnesium works in tandem with Calcium and Vitamin D; taking one without the others can actually disrupt mineral balance.
The Molecular Synergy: How Magnesium Repairs Musculoskeletal Tissue
To understand how magnesium “repairs” tissue, we must look at the cellular level. Magnesium acts as a natural calcium blocker. In the muscles, calcium triggers contraction, while magnesium facilitates relaxation. When a patient is deficient, muscles remain in a state of semi-contraction, leading to the cramps and chronic soreness often reported in athletic or aging populations.

In the skeletal system, magnesium is critical for the structural integrity of the bone matrix. It influences the activity of osteoblasts (cells that build bone) and osteoclasts (cells that break down bone). A deficiency doesn’t just lead to “weak” bones; it impairs the body’s ability to incorporate calcium into the bone, potentially increasing the risk of osteoporosis.
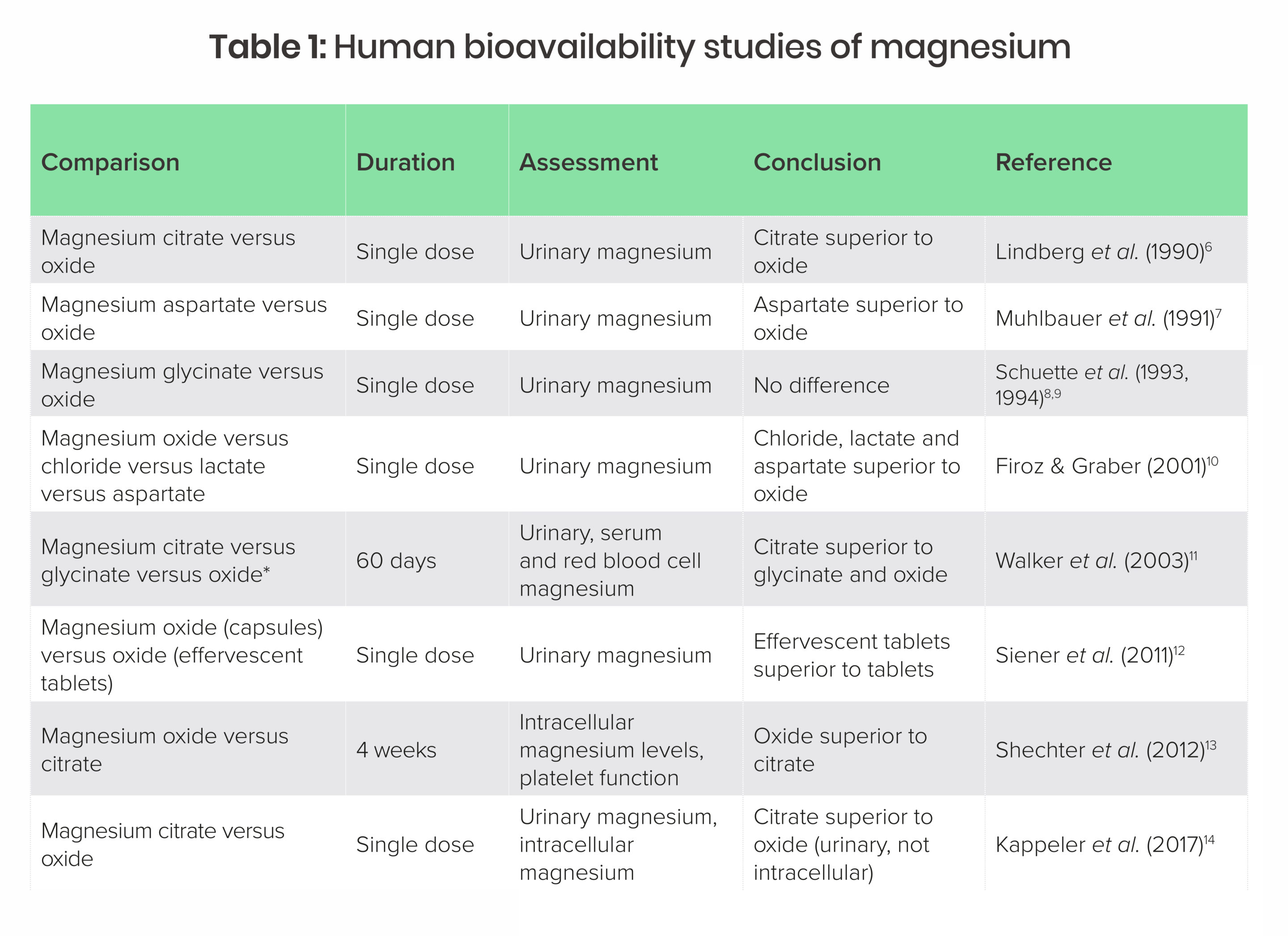
The double-blind placebo-controlled trials—the gold standard of research where neither the patient nor the doctor knows who is receiving the treatment—consistently show that correcting magnesium deficiency improves muscle function and bone mineral density. However, the efficacy is entirely dependent on the salt form used. For instance, organic chelates (magnesium bound to an amino acid) bypass many of the absorption hurdles found in inorganic salts.
| Magnesium Form | Primary Employ Case | Bioavailability | Common Side Effect |
|---|---|---|---|
| Magnesium Glycinate | Anxiety, Sleep, Nerve Health | Highly High | Minimal |
| Magnesium Malate | Fibromyalgia, Muscle Fatigue | High | Mild Digestive Upset |
| Magnesium Citrate | Constipation, General Deficiency | Moderate | Osmotic Laxative Effect |
| Magnesium Oxide | Heartburn, Occasional Constipation | Low | Diarrhea |
Global Regulatory Landscapes and Patient Access
The accessibility of these high-bioavailability forms varies significantly by region. In the United States, the FDA regulates magnesium as a dietary supplement rather than a drug, meaning purity and concentration can vary wildly between brands. This places the burden of quality control on the consumer.
In contrast, the European Medicines Agency (EMA) and various national health bodies in the EU often have stricter requirements for the “pharmaceutical grade” labeling of minerals. In the UK, the NHS typically focuses on dietary intake first, reserving supplementation for clinically diagnosed deficiencies (hypomagnesemia), whereas the US market pushes “wellness” supplementation even in the absence of a deficiency.
It is vital to note that most large-scale studies on magnesium are funded by independent academic institutions or government grants (such as the NIH), but the marketing of specific “proprietary blends” is often funded by supplement manufacturers. Patients should prioritize products with third-party certifications (like USP or NSF) to ensure the label matches the contents.
“The challenge in treating magnesium deficiency is not the availability of the mineral, but the precision of the delivery. We must move away from a ‘one size fits all’ approach to mineral supplementation and tailor the chelate to the patient’s specific metabolic need.” — Dr. Sarah Jenkins, PhD in Nutritional Epidemiology.
The Bioavailability Gap: Why Your Choice Matters
When a source mentions “repairing muscles,” they are often referring to the reduction of oxidative stress and the replenishment of intracellular magnesium levels. The mechanism of action here involves the stabilization of the cell membrane and the regulation of the sodium-potassium pump, which is essential for nerve impulse conduction.
Many consumers mistakenly purchase magnesium oxide because it is inexpensive. However, the absorption rate of oxide is roughly 4%, compared to over 25% for citrate and even higher for glycinate. From a public health perspective, this creates a “false sense of security” where patients believe they are treating a deficiency while the mineral is simply passing through their digestive tract.
For those focusing on bone health, the relationship between magnesium and Vitamin D is synergistic. Vitamin D cannot be metabolized without magnesium; specifically, the enzymes that convert Vitamin D into its active form (calcitriol) are magnesium-dependent. High-dose Vitamin D supplementation without adequate magnesium can actually deplete magnesium stores further, leading to a paradoxical increase in muscle tension.
Contraindications & When to Consult a Doctor
While magnesium is generally safe, it is not universal. Certain medical conditions make supplementation dangerous. The most critical contraindication is Renal Impairment (kidney disease). Because the kidneys are responsible for excreting excess magnesium, patients with chronic kidney disease (CKD) can develop hypermagnesemia, a potentially fatal condition where magnesium levels in the blood become too high, leading to respiratory depression and cardiac arrest.
Patients should consult a physician immediately if they experience:
- Extreme lethargy or muscle weakness.
- Irregular heartbeat (arrhythmia).
- Low blood pressure (hypotension).
magnesium can interfere with the absorption of certain medications, including tetracycline antibiotics and bisphosphonates (used for osteoporosis). Always maintain a two-hour window between taking these medications and a magnesium supplement.
The Path Forward: Evidence-Based Integration
As we move further into 2026, the trend toward “personalized nutrition” is becoming clinically grounded. The use of magnesium is shifting from a general wellness trend to a targeted therapeutic intervention. For those recovering from injury or managing age-related bone loss, the focus must remain on bioavailability and synergy.
The evidence is clear: repairing muscles and bones requires more than just a mineral; it requires the right chemical form and the right supporting nutrients. By prioritizing glycinates and malates and monitoring renal function, patients can safely optimize their musculoskeletal health without falling prey to supplement marketing hype.