
Breast cancer remains a leading cause of female mortality globally, often characterized by the deceptive presence of painless lumps. Early detection through clinical screening and biopsy is critical, as malignancy frequently develops without initial discomfort, significantly impacting five-year survival rates across diverse healthcare systems from the US to Southeast Asia.
The danger of breast cancer lies in its stealth. For many women, the first sign of a tumor is a palpable mass that does not cause pain, leading to a psychological “false security” where the absence of pain is mistaken for a lack of urgency. This delay in presentation often pushes the diagnosis from Stage I or II—where curative intent is high—to Stage III or IV, where the focus shifts toward palliative care and systemic management. In the current clinical landscape of April 2026, the integration of genomic profiling and AI-driven imaging is narrowing the gap in early detection, yet the fundamental necessity of physical awareness remains the first line of defense.
In Plain English: The Clinical Takeaway
- Pain is not a reliable indicator: Most malignant breast tumors are painless in their early stages; do not wait for pain to seek a medical evaluation.
- Screening saves lives: Regular mammograms or ultrasounds can discover tumors long before they can be felt by hand.
- Biopsy is the gold standard: If a lump is found, a biopsy (taking a little tissue sample) is the only way to definitively know if a growth is cancerous or benign.
The Pathophysiology of the “Painless Lump”: Why Malignancy Stays Silent
To understand why breast cancer often lacks pain, we must examine the mechanism of action—the specific biological process—of tumor growth. Most early-stage carcinomas grow slowly and do not initially compress nerve endings or trigger an inflammatory response. Pain typically occurs only when a tumor grows large enough to invade the surrounding chest wall, skin, or lymph nodes, or when it causes an infection.
Clinical pathology distinguishes between “benign” (non-cancerous) and “malignant” (cancerous) growths. A painless, hard, irregular lump with fixed borders is a classic red flag for malignancy. In contrast, cysts are often smooth, mobile, and may fluctuate in size or tenderness during the menstrual cycle. However, relying on “perceive” alone is clinically insufficient due to the overlap in physical characteristics.
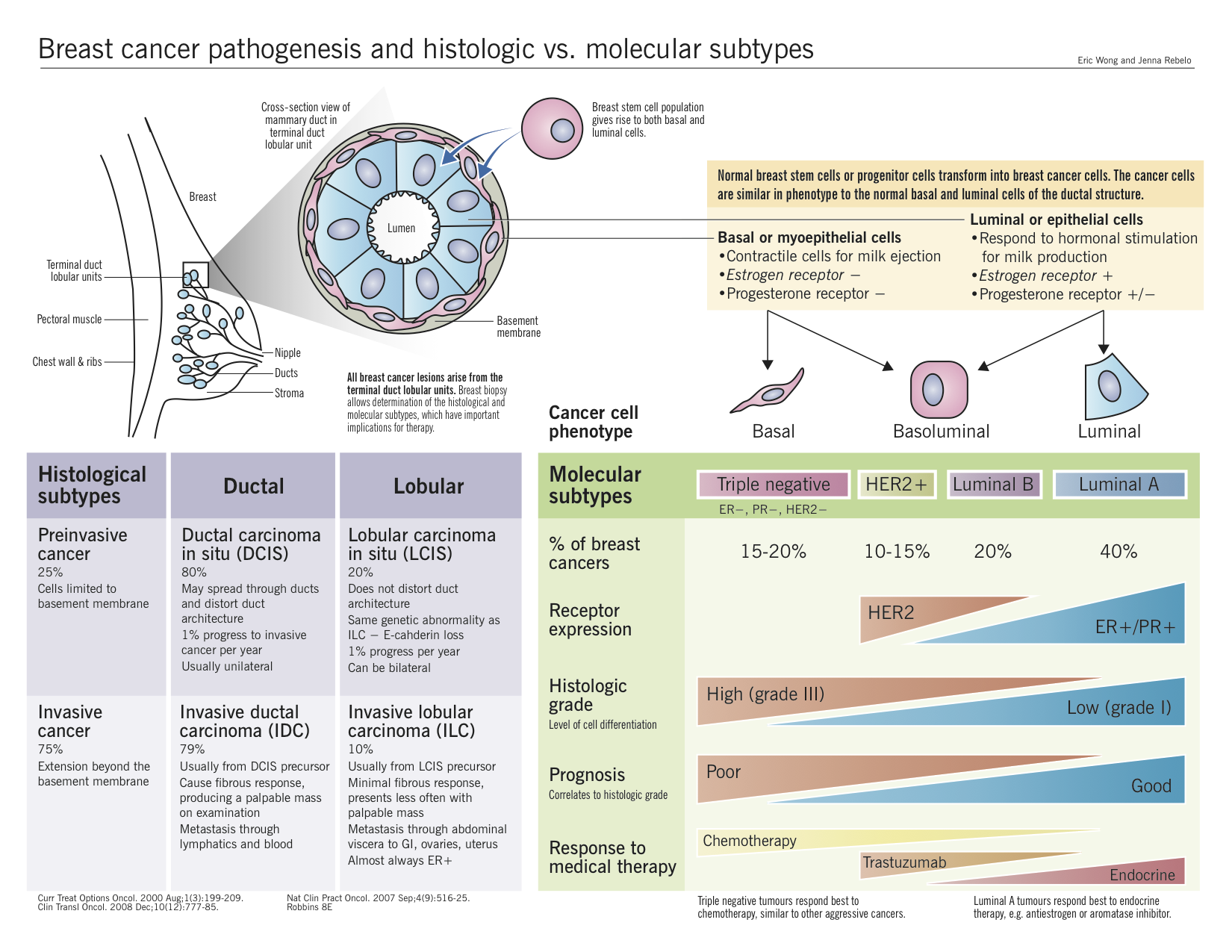
The molecular driver of many aggressive breast cancers is the overexpression of the HER2 protein, which signals the cell to grow and divide uncontrollably. This cellular proliferation happens silently at the microscopic level until a palpable mass forms. Current research published in The Lancet emphasizes that early intervention using targeted therapies can now neutralize these proteins, drastically improving outcomes if the cancer is caught before it metastasizes (spreads to other organs).
Global Screening Disparities: From the NHS to Emerging Healthcare Systems
The ability to detect a painless lump early is heavily dependent on the regional healthcare infrastructure. In the United Kingdom, the National Health Service (NHS) provides a centralized, invitation-based screening program that ensures high compliance. In the United States, the FDA oversees the approval of advanced 3D mammography (digital breast tomosynthesis), which increases the detection rate of small tumors in dense breast tissue.

However, a significant “information and access gap” exists in low-to-middle-income countries. In many regions, women rely solely on self-examination. Because they are conditioned to associate “sickness” with “pain,” the lack of discomfort leads to late-stage presentation. This geo-epidemiological divide results in a stark contrast in mortality rates; while survival is high in the West, it remains alarmingly low in regions where screening is not subsidized or accessible.
“The global disparity in breast cancer survival is not a failure of medicine, but a failure of delivery. We have the tools to detect and treat, but we lack the universal infrastructure to ensure every woman is screened before her cancer becomes symptomatic.” — Dr. Aruna Vasudevan, Global Health Epidemiologist.
To visualize the efficacy of different detection methods, the following table summarizes the clinical utility of current screening modalities:
| Modality | Primary Use Case | Sensitivity | Key Limitation |
|---|---|---|---|
| Mammography | General population screening | High (Moderate in dense breasts) | Radiation exposure; false positives |
| Ultrasound | Distinguishing cysts from solids | High for dense tissue | Operator dependent |
| MRI (Contrast) | High-risk patients/Genetic markers | Particularly High | High cost; lower specificity |
| Biopsy (Core Needle) | Definitive Diagnosis | Gold Standard (100%) | Invasive procedure |
The Evolution of Targeted Therapy and Funding Transparency
Modern oncology has moved beyond the “one size fits all” approach of systemic chemotherapy. We now utilize double-blind placebo-controlled trials—studies where neither the patient nor the doctor knows who is receiving the active drug—to validate targeted therapies. These include CDK4/6 inhibitors, which block specific proteins that help cancer cells divide.
It is vital to maintain journalistic transparency regarding the funding of these innovations. Much of the current research into HER2-positive and Triple-Negative Breast Cancer (TNBC) is funded by pharmaceutical entities such as Roche and Novartis, alongside government grants from the National Institutes of Health (NIH). While this funding drives rapid innovation, independent peer-review processes in journals like PubMed and JAMA are essential to ensure that efficacy data is not skewed by commercial interests.
The shift toward “Precision Medicine” means that a patient’s tumor is now sequenced to find its specific genetic mutation. This allows physicians to prescribe a drug that acts like a “key in a lock,” attacking only the cancer cells while sparing healthy tissue, thereby reducing the debilitating side effects associated with traditional chemotherapy.
Contraindications & When to Consult a Doctor
While screening is encouraged, certain contraindications—medical reasons why a specific treatment or test should not be used—apply. For instance, contrast-enhanced MRIs are contraindicated for patients with severe kidney dysfunction or certain metal implants. Similarly, hormone-replacement therapies (HRT) can increase the risk of certain breast cancers and should be monitored closely by an endocrinologist.
You must consult a healthcare provider immediately if you notice:
- A hard, painless lump in the breast or underarm area.
- Any change in the size or shape of the breast.
- Dimpling or puckering of the skin (resembling an orange peel).
- Nipple discharge other than breast milk, including blood.
- A newly inverted nipple (pulling inward).
The trajectory of breast cancer care is moving toward earlier, less invasive interventions. However, the most sophisticated AI and the most expensive targeted drugs are useless if the patient does not enter the clinic. The biological silence of a painless lump is the most dangerous symptom of all; vigilance and proactive screening remain the only definitive ways to change the global mortality statistics.
References
- World Health Organization (WHO) – Breast Cancer Fact Sheets
- The Lancet – Global Burden of Cancer Studies
- PubMed – National Center for Biotechnology Information (NCBI)
- JAMA – Journal of the American Medical Association
- American Cancer Society (ACS) – Screening Guidelines 2025-2026