
Colorectal cancer remains the second most frequent malignancy in Argentina and a leading cause of oncological death globally. As we observe World Colon Cancer Day on March 31, 2026, a critical epidemiological shift demands attention: incidence rates are rising sharply in adults under the age of 50. This article synthesizes current clinical consensus on early-onset colorectal cancer, detailing the biological mechanisms linking lifestyle to tumorigenesis and outlining evidence-based prevention strategies.
Historically categorized as a disease of aging, colorectal cancer (CRC) is undergoing a demographic transformation that challenges standard screening protocols. While 70% of cases still occur in individuals over 70, the relative proportion of diagnoses in younger populations has escalated over the last decade. This trend, observed in high-income nations and increasingly in developing economies, suggests that environmental and lifestyle factors—specifically the “Westernization” of diet and sedentary behavior—are accelerating carcinogenesis in genetically susceptible individuals. Understanding this pivot is essential for patients and providers to adjust triage thresholds and prevent avoidable mortality.
In Plain English: The Clinical Takeaway
- Screening Age Has Shifted: Preventative screening is now recommended to begin at age 45 for average-risk individuals, not 50, to catch precancerous polyps earlier.
- Symptoms Are Not “Normal”: Persistent changes in bowel habits, unexplained anemia, or blood in the stool require immediate investigation, regardless of age.
- Lifestyle is Medicine: Reducing ultra-processed foods and increasing fiber intake directly lowers inflammation in the colon, reducing the risk of malignant transformation.
The Microbiome and the “Western Diet” Hypothesis
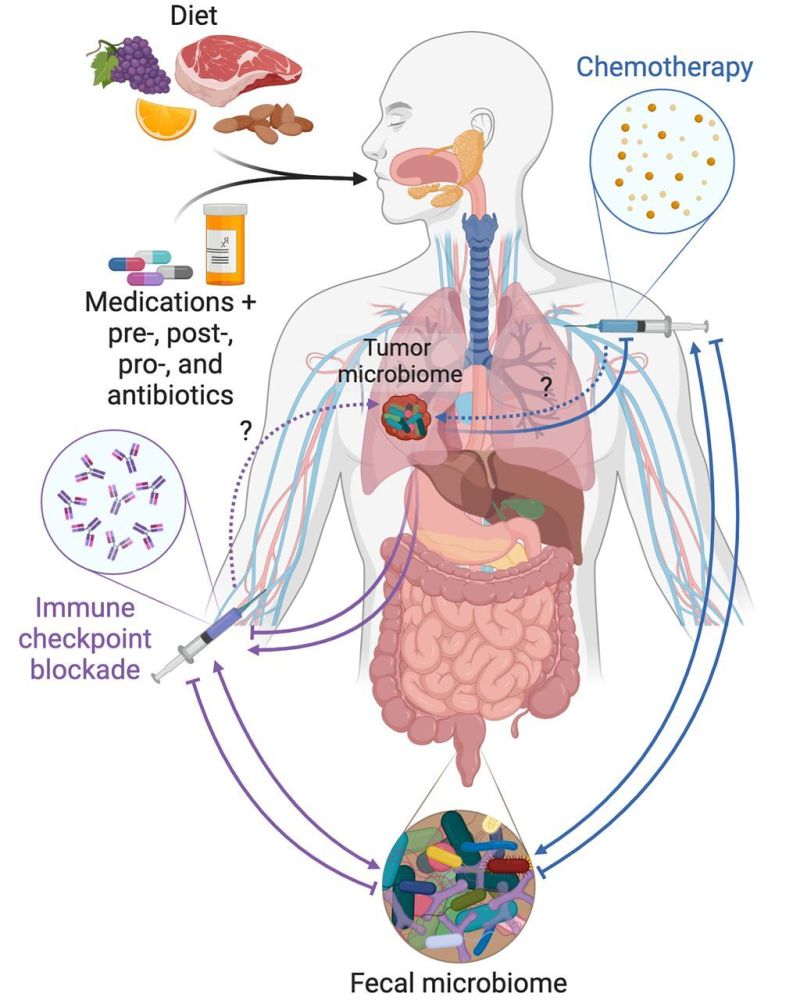
The source material correctly identifies sedentary behavior and ultra-processed foods as risk factors, but the clinical mechanism requires deeper explanation. Current research in 2026 points strongly toward the gut microbiome as a mediator between diet and cancer. Diets high in red meat and low in fiber alter the bacterial composition of the colon, promoting the growth of pro-inflammatory species such as Fusobacterium nucleatum. This bacterium has been shown to adhere to colorectal tumor cells and suppress the local immune response, effectively creating a microenvironment where adenomatous polyps—precursors to cancer—can evolve into malignancies more rapidly.
the rise in early-onset cases is disproportionately affecting the left side of the colon and the rectum. This anatomical specificity is significant because left-sided tumors often present with obstructive symptoms or visible bleeding earlier than right-sided tumors, yet they are frequently misdiagnosed in young adults as hemorrhoids or irritable bowel syndrome (IBS). This diagnostic delay, often spanning six to nine months from symptom onset to biopsy, allows the disease to progress to advanced stages where curative resection is more complex.
“We are seeing a generational shift in cancer biology. The increase in early-onset colorectal cancer is not just a statistical anomaly; it reflects a fundamental change in how our environment interacts with our genetics. The latency period for colon cancer is typically 10 to 15 years, meaning the exposures driving today’s diagnoses in 40-year-olds began in their adolescence.” — Dr. Rebecca Siegel, Senior Scientist at the American Cancer Society
Global Screening Protocols and Regulatory Divergence
Prevention relies heavily on the removal of precancerous polyps via colonoscopy. In the United States, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended screening age from 50 to 45 in 2021, a guideline that has become the standard of care in 2026. However, regulatory bodies in Europe (EMA) and Latin America are navigating different resource landscapes. While the clinical evidence supports earlier screening, implementation varies based on healthcare infrastructure.
In Argentina, where the source indicates CRC is the second most frequent tumor, the challenge is twofold: increasing awareness among young adults who do not perceive themselves as “at risk,” and ensuring access to colonoscopy, which remains the gold standard. Non-invasive alternatives, such as the Fecal Immunochemical Test (FIT), offer a viable bridge for populations with limited endoscopic access. FIT detects hidden blood in the stool with high specificity for human hemoglobin, serving as an effective triage tool to prioritize who needs a colonoscopy.
The following table summarizes the efficacy and application of current screening modalities recommended for the 2026 clinical landscape:
| Screening Modality | Frequency | Primary Mechanism | Clinical Utility |
|---|---|---|---|
| Colonoscopy | Every 10 years | Direct visualization and polyp removal | Gold Standard; Preventative and Diagnostic |
| FIT (Fecal Immunochemical Test) | Annually | Detection of hidden blood | High accessibility; requires follow-up colonoscopy if positive |
| Stool DNA Test (e.g., Cologuard) | Every 3 years | Detection of altered DNA and blood | Higher sensitivity for cancer, lower for advanced polyps |
| CT Colonography | Every 5 years | 3D imaging of the colon | Non-invasive; requires bowel prep; radiation exposure |
Contraindications & When to Consult a Doctor
While lifestyle modification is universally beneficial, specific clinical scenarios require immediate professional intervention rather than self-management. Patients should not rely on “wait and see” approaches if they present with “alarm symptoms.” These include rectal bleeding that persists beyond two weeks, unexplained iron-deficiency anemia (which may manifest as fatigue or pallor), unintentional weight loss, or a persistent change in stool caliber (pencil-thin stools).
Contraindications for certain screening methods likewise exist. For instance, patients with active inflammatory bowel disease (such as Crohn’s disease or Ulcerative Colitis) require a different surveillance protocol, often starting at the time of diagnosis rather than age 45, due to their elevated risk profile. Those with a family history of colorectal cancer or hereditary syndromes like Lynch Syndrome should consult a genetic counselor. For these high-risk groups, screening may require to commence as early as age 20 or 10 years prior to the youngest relative’s age at diagnosis.
The Path Forward: Multidisciplinary Care
The management of colorectal cancer has evolved into a highly personalized endeavor. As noted by specialists at the Alexander Fleming Institute, the integration of immunotherapy and targeted therapies has improved outcomes for metastatic disease. However, the most potent tool remains primary prevention. The correlation between chronic non-communicable diseases (such as type 2 diabetes and obesity) and CRC underscores that metabolic health is inextricably linked to oncological risk.
As we mark this World Colon Cancer Day, the medical community’s directive is clear: we must destigmatize colon screening and recognize that age is no longer a shield against this disease. By adopting a diet rich in whole grains and vegetables, maintaining a healthy weight and adhering to updated screening guidelines, the trajectory of this epidemic can be altered. Early detection does not just save lives; it preserves the quality of life by allowing for less invasive treatments and higher cure rates.
References
- Siegel, R. L., et al. (2025). “Colorectal cancer statistics, 2025.” CA: A Cancer Journal for Clinicians. American Cancer Society.
- U.S. Preventive Services Task Force. (2021). “Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement.” JAMA.
- World Health Organization. (2026). “Global Cancer Observatory: Colorectal Cancer Fact Sheet.” WHO/IARC.
- Brenner, H., et al. (2024). “Long-term effects of colorectal cancer screening on incidence and mortality.” The Lancet Gastroenterology & Hepatology.
- National Cancer Institute. (2026). “Colorectal Cancer Prevention (PDQ®)–Health Professional Version.” NIH.