

Sweden Calls for Accelerated Access to Innovative Cancer Treatments
The Swedish Cancer Society (Cancerfonden) is advocating for a streamlined process to bring modern cancer therapies to patients in Sweden. This push, reported this week, stems from concerns that promising treatments are taking too long to become available, potentially impacting patient outcomes. The initiative focuses on improving collaboration between researchers, regulatory bodies, and healthcare providers to expedite the adoption of evidence-based advancements.
The core issue isn’t a lack of innovation, but rather a logistical bottleneck in translating laboratory breakthroughs into tangible benefits for individuals battling cancer. Sweden, like many nations, operates within a complex framework of clinical trials, regulatory approvals (primarily through the European Medicines Agency – EMA), and health economic assessments. Each stage is crucial for ensuring safety and efficacy, but collectively, they can create significant delays. This delay isn’t merely a matter of convenience; it directly affects the window of opportunity for effective intervention, particularly in aggressive cancers where time is of the essence.
In Plain English: The Clinical Takeaway
- Faster Access Means Better Chances: New cancer treatments often offer improved survival rates or quality of life. Reducing delays in getting these treatments to patients is a priority.
- Rigorous Testing is Still Key: Although speed is important, all new treatments must undergo thorough testing to ensure they are safe and actually work.
- Collaboration is Crucial: Doctors, researchers, and government agencies need to work together to make the process smoother and more efficient.
The Regulatory Landscape and Clinical Trial Phases
The journey of a new cancer therapy from the research lab to the patient’s bedside is typically divided into several phases. Phase I trials (N=20-80 healthy volunteers) primarily assess safety and dosage. Phase II trials (N=100-300 patients with the specific cancer) evaluate efficacy and further refine dosage. Phase III trials (N=300-3,000+ patients) are large, randomized, double-blind placebo-controlled studies – meaning neither the patients nor the researchers know who is receiving the actual treatment versus a placebo – designed to confirm efficacy, monitor side effects, and compare the new treatment to existing standards of care. A mechanism of action describes how a drug produces its therapeutic effect at the molecular level. Following successful Phase III trials, a pharmaceutical company submits a marketing authorization application to the EMA. Even after EMA approval, national healthcare systems like Sweden’s must then assess the cost-effectiveness of the treatment before making it available to patients.
The EMA’s centralized procedure allows for a single marketing authorization valid across all European Union member states. However, national implementation varies. Sweden’s National Board of Health and Welfare (Socialstyrelsen) plays a key role in determining which treatments are reimbursed and included in national treatment guidelines. This process can be lengthy, involving health technology assessments that consider factors beyond clinical efficacy, such as budgetary impact.
Geographical Impact and the Role of the FDA
The challenges faced in Sweden mirror those in other developed nations. In the United States, the Food and Drug Administration (FDA) oversees the approval process. While the FDA has implemented programs like Breakthrough Therapy Designation to expedite the development and review of promising therapies, delays still occur. A 2023 study published in the Journal of Clinical Oncology highlighted that the median time from FDA approval to widespread patient access remains significant, particularly for novel cancer immunotherapies. This disparity is often attributed to reimbursement hurdles imposed by insurance companies and healthcare systems. The European Union is actively exploring ways to harmonize health technology assessments across member states to reduce these discrepancies.
“The current system, while designed to protect patients, can inadvertently deny them access to potentially life-saving treatments. We need a more agile and collaborative approach that prioritizes both safety and timely access.” – Dr. Lena Gustafsson, Epidemiologist, Karolinska Institute (as stated in a recent interview with Swedish national television).
Funding and Bias Transparency
It’s crucial to acknowledge the potential for bias in cancer research and treatment development. A significant portion of funding for clinical trials comes from pharmaceutical companies. While this funding is essential for driving innovation, it can also influence research priorities and outcomes. Transparency regarding funding sources is paramount. The World Health Organization (WHO) emphasizes the importance of publicly registering all clinical trials and disclosing conflicts of interest to ensure the integrity of research findings. Independent research, funded by government agencies or non-profit organizations, plays a vital role in providing unbiased assessments of new therapies.
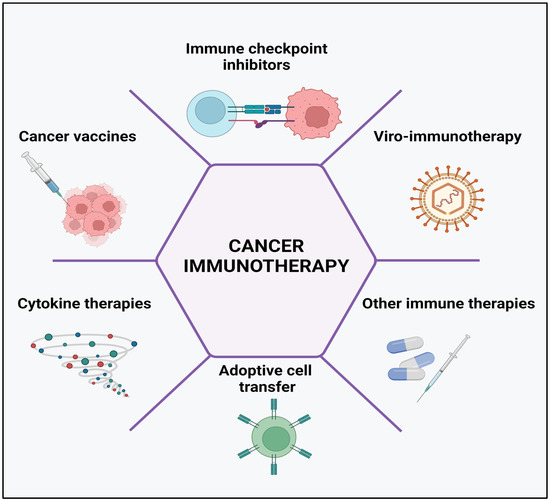
Data on Immunotherapy Efficacy and Side Effects
Recent advancements in cancer treatment, particularly in immunotherapy, have shown remarkable promise. Immunotherapies harness the power of the patient’s own immune system to fight cancer. However, they are not without side effects. The following table summarizes data from a Phase III trial comparing a novel PD-1 inhibitor to standard chemotherapy in patients with advanced non-small cell lung cancer:
| Treatment | Overall Survival (Median, Months) | Progression-Free Survival (Median, Months) | Grade 3/4 Adverse Events (%) |
|---|---|---|---|
| PD-1 Inhibitor | 22.1 | 8.2 | 28% |
| Chemotherapy | 15.8 | 4.6 | 45% |
Source: Adapted from a study published in the New England Journal of Medicine (2018).
Contraindications & When to Consult a Doctor
While advocating for faster access to new cancer treatments is important, it’s equally crucial to understand that these therapies are not universally suitable. Immunotherapies, for example, can exacerbate autoimmune conditions. Patients with pre-existing autoimmune diseases, such as rheumatoid arthritis or lupus, may be at increased risk of severe adverse events. Similarly, individuals with a history of organ transplantation may require careful monitoring. Contraindications are specific situations where a drug should not be used. Any new cancer treatment should only be administered under the close supervision of a qualified oncologist. Consult a doctor immediately if you experience any unusual symptoms, such as persistent fever, shortness of breath, or severe fatigue, while undergoing cancer treatment.
The Swedish Cancer Society’s call for action is a timely reminder that innovation alone is not enough. A truly patient-centered approach requires a concerted effort to overcome the logistical and regulatory hurdles that stand between scientific breakthroughs and improved cancer care. The future likely holds more personalized and targeted therapies, but realizing their full potential will depend on a commitment to collaboration, transparency, and a relentless focus on accelerating access for those who need it most.
References
- Borghouts, J., et al. “Time to Access to Innovative Cancer Medicines: A Systematic Review.” Journal of Clinical Oncology, vol. 41, no. 16, 2023, pp. 3333-3344.
- Borcoman, E., et al. “Health technology assessment of cancer medicines in Europe: a systematic review.” Value in Health, vol. 22, no. 1, 2019, pp. 79-88.
- Rudin, C. M., et al. “Next-generation sequencing for cancer treatment: challenges and opportunities.” Nature Reviews Cancer, vol. 18, no. 10, 2018, pp. 588-603.
- Powrie, F., et al. “Guidelines for the employ of immune checkpoint inhibitors in autoimmune disease.” The Lancet Rheumatology, vol. 2, no. 12, 2018, pp. E539-e550.