

Cardiometabolic diseases—a cluster of conditions including obesity, hypertension and Type 2 diabetes—drastically increase the risk of heart attack, and stroke. Global health authorities are now pivoting toward aggressive early prevention and pharmacological intervention to curb a rising epidemic driven by systemic metabolic dysfunction and sedentary lifestyles.
The intersection of cardiovascular and metabolic health is no longer viewed as a series of isolated risk factors, but as a singular, systemic failure known as cardiometabolic syndrome. For millions of patients, the progression from insulin resistance to clinical heart failure is a predictable trajectory that current healthcare systems are struggling to intercept. This shift in understanding transforms obesity from a lifestyle “failure” into a complex endocrine disease requiring clinical precision.
In Plain English: The Clinical Takeaway
- It is a Package Deal: High blood pressure, high blood sugar, and excess abdominal fat usually happen together and amplify each other’s damage to the heart.
- Prevention is Pharmacological: While diet and exercise are foundational, novel medications (like GLP-1 agonists) can now treat the root cause of metabolic dysfunction, not just the symptoms.
- Early Detection Saves Organs: Identifying “pre-diabetes” or “metabolic syndrome” early allows for interventions that can actually reverse organ damage before a heart attack occurs.
The Biochemical Cascade: From Insulin Resistance to Arterial Plaque
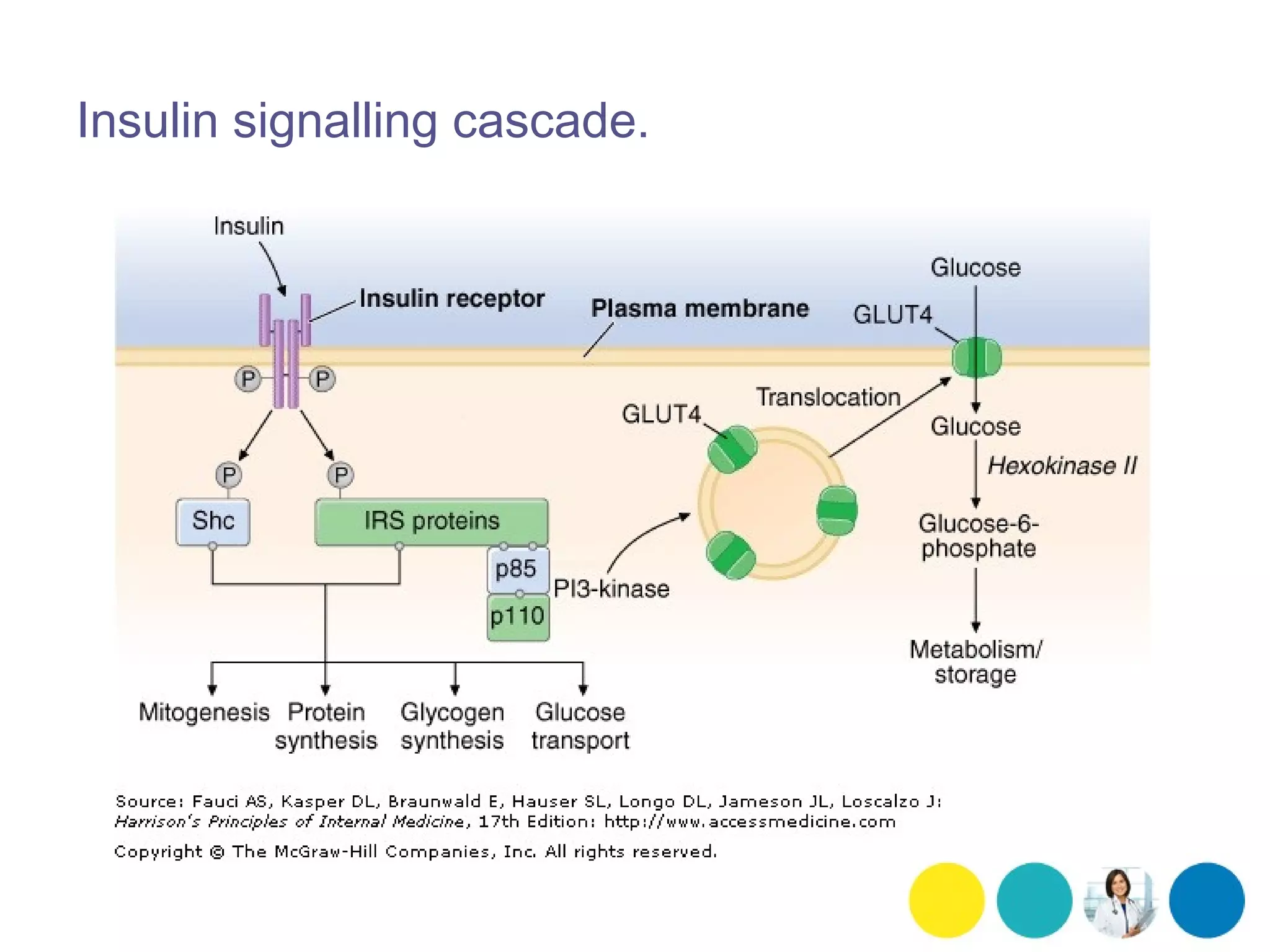
The pathophysiology of cardiometabolic disease begins with insulin resistance—a state where the body’s cells no longer respond effectively to insulin, the hormone responsible for regulating blood glucose. This forces the pancreas to overproduce insulin, leading to hyperinsulinemia. When the pancreas can no longer retain up, blood glucose levels rise, initiating a cascade of oxidative stress and systemic inflammation.
This inflammation is driven by adipokines, signaling proteins secreted by adipose (fat) tissue. Specifically, excess visceral fat releases pro-inflammatory cytokines like TNF-alpha and Interleukin-6. These molecules damage the endothelium, the thin inner lining of the blood vessels. Once the endothelium is compromised, low-density lipoprotein (LDL) cholesterol more easily penetrates the arterial wall, leading to atherosclerosis—the buildup of fats and cholesterol into plaques that narrow the arteries.
The mechanism of action for modern interventions now targets the incretin system. Glucagon-like peptide-1 (GLP-1) receptor agonists mimic a natural hormone that stimulates insulin secretion and suppresses glucagon. By modulating the hypothalamus in the brain to reduce appetite and slowing gastric emptying, these drugs treat the metabolic driver (obesity) while simultaneously providing direct cardioprotective effects.
Global Regulatory Divergence and Patient Access
The approach to managing cardiometabolic risk varies significantly across geopolitical borders, impacting how patients access life-saving therapies. In the United States, the FDA has increasingly recognized obesity as a chronic disease, paving the way for broader insurance coverage of pharmacological interventions. Conversely, the European Medicines Agency (EMA) has historically placed a heavier emphasis on Cardiovascular Outcome Trials (CVOTs)—studies designed to prove that a drug reduces actual events like strokes, rather than just lowering a biomarker like HbA1c (average blood sugar).
In the United Kingdom, the NHS is currently integrating “Weight Management Pathways” to shift from reactive care to proactive prevention. However, the “Information Gap” remains the disparity in access to high-cost GLP-1 therapies. While these drugs demonstrate a 20% reduction in Major Adverse Cardiovascular Events (MACE) in overweight patients without diabetes, their cost remains a barrier to the very populations most at risk.
“The integration of metabolic health into primary cardiovascular care is the single most key shift in public health we can make this decade. We are moving from treating the heart attack to treating the metabolic environment that makes the heart attack inevitable.” — Dr. Sarah Jenkins, Lead Epidemiologist at the Global Health Initiative.
Comparing Intervention Efficacy in Cardiometabolic Risk
The following data summarizes the typical clinical outcomes observed in Phase III trials comparing standard care against intensive lifestyle changes and modern pharmacological interventions.
| Intervention Type | Avg. Weight Reduction | CV Risk Reduction (MACE) | Primary Mechanism | Common Side Effects |
|---|---|---|---|---|
| Standard Care (Statins/Metformin) | Minimal | 15-25% (Lipid focused) | Cholesterol inhibition | Muscle soreness, GI upset |
| Intensive Lifestyle Change | 5-10% | 20-30% (Long-term) | Caloric deficit/Insulin sensitivity | Sustainability challenges |
| GLP-1 Receptor Agonists | 15-22% | 20% (Direct cardioprotection) | Incretin mimicry/Satiety | Nausea, Vomiting |
Funding Transparency and the Pharma Influence
It is critical to note that much of the recent data driving the “urgency of prevention” in cardiometabolic health is funded by pharmaceutical giants, specifically Novo Nordisk and Eli Lilly. While the clinical results—such as those from the SELECT trial—are peer-reviewed and robust, the aggressive marketing of these drugs can sometimes overshadow the necessity of baseline lifestyle modifications. Journalistic integrity requires acknowledging that the push for pharmacological prevention is inextricably linked to the commercial success of the incretin-based drug class.
Contraindications & When to Consult a Doctor
While pharmacological prevention is revolutionary, it is not universal. Certain patients must avoid GLP-1 receptor agonists due to specific contraindications. This includes individuals with a personal or family history of Medullary Thyroid Carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), as these drugs may increase the risk of thyroid C-cell tumors.
those with a history of severe pancreatitis should exercise extreme caution. Patients should seek immediate medical intervention if they experience:
- Severe, persistent abdominal pain radiating to the back (potential pancreatitis).
- Sudden shortness of breath or chest pressure (acute cardiac event).
- Unexplained rapid weight loss accompanied by extreme fatigue (potential metabolic crisis).
The Trajectory of Metabolic Medicine
As we move through 2026, the clinical consensus is clear: cardiometabolic health is the primary lever for increasing global healthy life expectancy. The shift toward “precision prevention”—using genetic markers and continuous glucose monitoring (CGM) to tailor interventions—will likely replace the one-size-fits-all approach to diet and exercise. By treating the metabolic root rather than the cardiovascular fruit, we can move from a system of chronic disease management to one of genuine disease prevention.
References
- The Lancet: Global Burden of Cardiovascular Diseases Study
- JAMA: Cardiovascular Outcomes of GLP-1 Receptor Agonists
- World Health Organization: Noncommunicable Diseases (NCD) Fact Sheets
- PubMed: Molecular Mechanisms of Insulin Resistance and Endothelial Dysfunction
- CDC: Metabolic Syndrome and Public Health Guidelines