
{kind=link}
“`html
Rare Autoimmune blistering Disease Presents Unique Challenges For Doctors
Table of Contents
- 1. Rare Autoimmune blistering Disease Presents Unique Challenges For Doctors
- 2. Understanding Autoimmune Diseases And Blistering Skin Conditions
- 3. Frequently Asked Questions About Bullous Pemphigoid
- 4. What Is Idiopathic Bullous Pemphigoid?
- 5. What Are The Common Symptoms Of Bullous Pemphigoid?
- 6. How Is Bullous Pemphigoid Diagnosed?
- 7. What Are The Treatment Options For Bullous Pemphigoid?
- 8. Is Bullous Pemphigoid A Serious Condition?
- 9. Can Bullous Pemphigoid Affect The Mouth?
- 10. What Causes Idiopathic Bullous Pemphigoid?
- 11. Okay,here’s a breakdown of the provided case study,focusing on key data and potential questions it might be used to assess understanding. I’ll organize it into sections: **Summary, Key Findings, Differential Diagnosis Considered, Diagnostic Steps & Results, and Potential Discussion Points/Questions.**
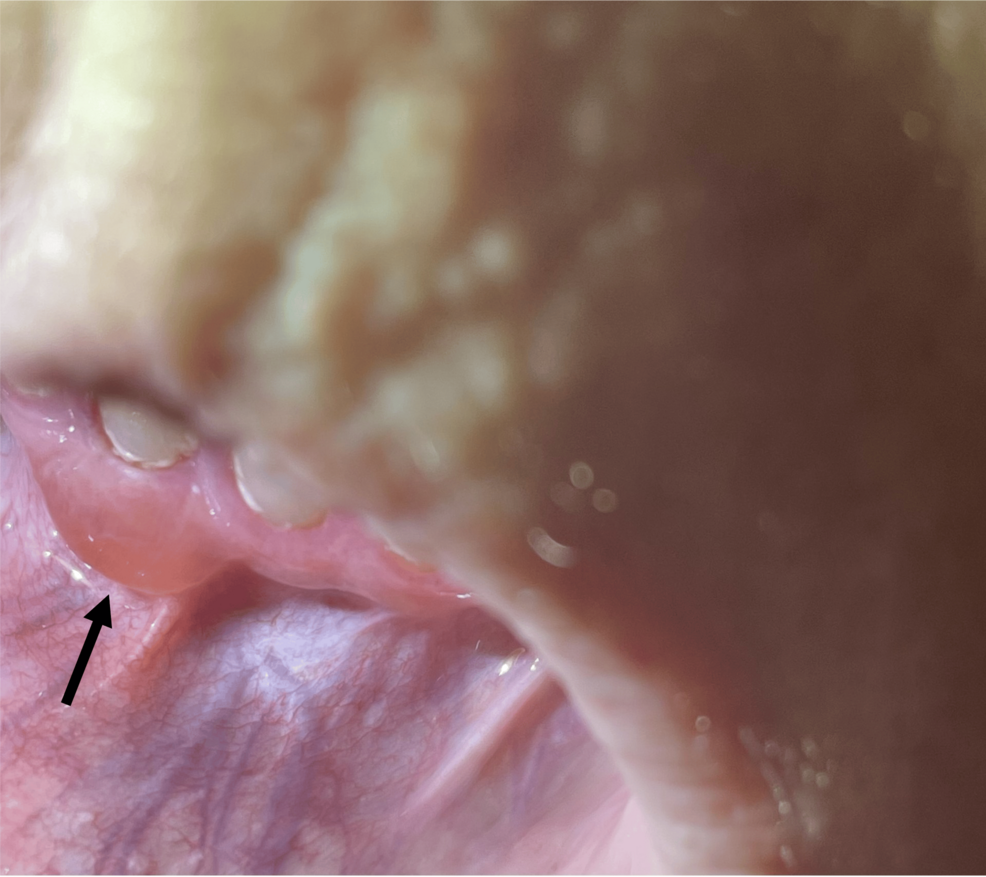
- 12. Case Study: Concurrent Gingival and Cutaneous Involvement in Idiopathic Bullous Pemphigoid
- 13. Understanding Bullous Pemphigoid: A Deep Dive
- 14. Case Presentation: A 78-year-Old Female
- 15. Diagnostic workup: Confirming the Diagnosis
- 16. Treatment and Management: A Multi-faceted Approach
- 17. Monitoring and Follow-up
- 18. The Importance of Early and accurate Diagnosis
- 19. Benefits of Recognizing Concurrent Presentation
- 20. practical Tips for Clinicians
A Recently Published Case Report Highlights The Complexity Of Diagnosing And Treating Idiopathic Bullous Pemphigoid.
Doctors Are Increasingly Aware Of The Challenges Posed By Rare Autoimmune Diseases. A New Case Report Published In Curet Details A Complex Presentation Of Idiopathic Bullous Pemphigoid (IBP), A Rare Blistering Skin Condition. The Case Involved A Patient Exhibiting Both Oral And Skin Manifestations, Complicating The Diagnostic Process.
Idiopathic Bullous Pemphigoid Occurs When The Immune System Mistakenly Attacks A Layer Of Skin Tissue. This Leads To The Formation Of Blisters, Typically In Older Adults. However, The Recent Case Demonstrates That The Disease Can Present atypical Symptoms, requiring Vigilance From Healthcare Professionals.
The PatientS condition Involved Blisters In The Mouth (Gingival Involvement) Alongside Those On The Skin. this Concurrent Presentation Is Not Typical And Delayed Initial Diagnosis. Accurate And Timely Diagnosis Is Crucial For Effective treatment And To Prevent Potential Complications.
Treatment For IBP Usually Involves Corticosteroids And Immunosuppressant Medications. These Medications Help To Suppress The Immune System And Reduce Inflammation. The Case Report Emphasizes The Importance Of A Personalized Treatment approach, Tailored To The Specific Needs Of Each Patient.
Understanding Autoimmune Diseases And Blistering Skin Conditions
Autoimmune Diseases Affect Millions Worldwide. These Conditions Arise When The Immune System Attacks The Body’s Own Tissues. Blistering Skin Diseases, Like Bullous Pemphigoid, Are Often A Manifestation Of These Underlying Immune System Dysfunctions.
Early Recognition Of Symptoms Is Key. Common Signs Include Blisters, Itching, And Skin Inflammation. While Many Skin Conditions Cause Blisters,Persistent Or Widespread Blistering Should Prompt A Medical Evaluation. Prompt Diagnosis Can Lead To More Effective Management And Improved Quality Of Life.
Researchers Continue To Investigate The Causes And Potential Cures For Autoimmune Diseases. Current Research Focuses On Developing More Targeted Therapies Wiht Fewer Side Effects. Staying Informed About The Latest Advances In Medical Science Is Essential For Both Patients And Healthcare Providers.
Frequently Asked Questions About Bullous Pemphigoid
-
What Is Idiopathic Bullous Pemphigoid?
It Is A Rare Autoimmune Disease That Causes Blisters On the Skin And mucous Membranes, Often Affecting Older Adults.
-
What Are The Common Symptoms Of Bullous Pemphigoid?
Symptoms Include Itchy, blistered Skin, Typically On The Arms, Legs, And Torso. Blisters Can Also Occur In The Mouth.
-
How Is Bullous Pemphigoid Diagnosed?
Diagnosis Usually Involves A Skin Biopsy To Examine The Tissue under A Microscope And Identify Specific antibodies.
-
What Are The Treatment Options For Bullous Pemphigoid?
Treatment Typically Involves Corticosteroids And Immunosuppressant Medications To suppress The Immune System.
-
Is Bullous Pemphigoid A Serious Condition?
While Not Typically Life-threatening, Bullous Pemphigoid Can Cause Notable Discomfort and Complications If Left Untreated.
-
Can Bullous Pemphigoid Affect The Mouth?
Yes, oral Involvement, Affecting The Gingiva And mucous membranes, Can Occur in certain specific cases.
-
What Causes Idiopathic Bullous Pemphigoid?
The Exact Cause Is Unknown, But It Is Believed To Be An Autoimmune Reaction Were The Body Attacks Its Own skin tissue.