
{kind=link}
A groundbreaking treatment for a challenging medical condition is gaining attention within the gastroenterological community. doctors have successfully employed a percutaneous transvenous retrograde embolization technique to address small bowel varices linked to abdominal adhesions, offering a potential option to more extensive surgical interventions.
Understanding Small Bowel Varices and Adhesions
Small bowel varices, abnormal and enlarged veins in the small intestine, can lead to notable gastrointestinal bleeding and are often challenging to manage. Thes can arise as a complication of portal hypertension, but are less common than varices in the esophagus. When these varices are connected to prior surgical adhesions – bands of scar tissue that can form after abdominal surgery – treatment becomes even more complex. adhesions can constrict blood flow and exacerbate the problem.
According to the National institutes of Health (NIH),roughly 90% of people who have abdominal surgery develop adhesions. However, only a small percentage of these adhesions lead to complications like small bowel varices.
the Percutaneous Transvenous Retrograde Embolization Procedure
The recently reported case details a patient who underwent a percutaneous transvenous retrograde embolization. This minimally invasive procedure involves accessing the veins through the skin, navigating to the affected varices, and then using embolic agents – substances that block blood flow – to stop the bleeding. The procedure aims to selectively target the problematic veins while preserving the surrounding healthy tissue. This contrasts with more radical surgical approaches that may be necessary in some cases.
The key benefit of this technique is its reduced risk profile compared to customary surgery. Patients typically experience less pain, shorter hospital stays, and a faster recovery time.It’s notably favorable for individuals who are not ideal candidates for more invasive procedures due to underlying health conditions.
How the Procedure works: A Step-by-Step Look
the procedure generally involves several key steps:
- A small incision is made to access a vein.
- Using imaging guidance, a catheter is guided through the veins to the varices.
- A contrast dye is injected to visualize the varices.
- Embolic agents are delivered to block blood flow.
- Imaging is used to confirm prosperous embolization.
Did You Know? Embolization techniques are not new, but their application to adhesion-related small bowel varices represents an innovative approach.
Comparative Treatment Options for Small Bowel Varices
Here’s a comparison of common treatment approaches:
| Treatment Option | Invasiveness | Recovery Time | Potential Risks |
|---|---|---|---|
| Surgery | High | Weeks to Months | Infection, Bleeding, Bowel Obstruction |
| Endoscopic Therapy | Moderate | Days to Weeks | Bleeding, Perforation |
| Percutaneous Embolization | Low | Days | Bleeding, Infection |
pro Tip: Early diagnosis and intervention are crucial for managing small bowel varices and preventing life-threatening complications.
Future Implications and Research
While this case report highlights a promising development, further research is needed to establish the efficacy and long-term outcomes of percutaneous transvenous retrograde embolization for adhesion-related small bowel varices. Larger studies are essential to confirm its safety and refine the technique. Experts believe that this approach could become a valuable addition to the arsenal of tools available for treating this complex condition.
Are there new advancements in minimally invasive procedures that could change the landscape of gastroenterological care? What role will imaging technology play in improving the precision of these types of interventions?
Understanding Adhesions: Prevention and Management
Even tho adhesions can’t always be prevented, certain surgical techniques and postoperative care protocols can minimize their formation.These include meticulous surgical technique, the use of adhesion barriers, and early mobilization of patients after surgery. Managing existing adhesions frequently enough involves pain management and, in certain specific cases, surgical intervention when they cause complications like bowel obstruction or varices.
Frequently Asked Questions About Small Bowel Varices and Embolization
- What are small bowel varices? They are enlarged veins in the small intestine that can cause bleeding.
- What causes adhesion-related small bowel varices? They develop as a complication of adhesions formed after abdominal surgery.
- What is percutaneous transvenous retrograde embolization? It’s a minimally invasive procedure to block bleeding from varices.
- Is this procedure widely available? Currently, it’s not widely available and requires specialized expertise.
- What are the risks of embolization? Potential risks include bleeding and infection.
- What is the recovery time after embolization? Typically, recovery is relatively swift, taking only a few days.
- How can I prevent adhesions after surgery? Meticulous surgical technique and early mobilization can definitely help reduce the risk.
Share your thoughts on this medical breakthrough in the comments below! Do you think minimally invasive procedures are the future of gastroenterological care?
What are teh key diagnostic modalities used to identify small bowel varices, and what are their respective limitations?
Case Study: Management of Small Bowel Varices with Percutaneous Transvenous Retrograde Embolization: An Adhesion-Related Intervention
Understanding Small Bowel Varices & Their Challenges
small bowel varices (SBV) are dilated veins within the wall of the small intestine, typically arising as a outcome of portal hypertension. Unlike esophageal varices, SBV are rarer and present a diagnostic and therapeutic challenge due to their location and the risk of significant bleeding. Customary management options, including surgery, carry significant morbidity and mortality. Percutaneous Transvenous Retrograde Embolization (PTRE) has emerged as a valuable, minimally invasive alternative, particularly when adhesion-related complications arise. This case study details a complex SBV management scenario highlighting the importance of recognizing and addressing adhesion formation during the procedure. Keywords: small bowel varices, portal hypertension, PTRE, embolization, adhesion, mesenteric vein, variceal bleeding.
Diagnostic Approach to Small Bowel Varices
Accurate diagnosis is paramount. Initial suspicion ofen arises from unexplained gastrointestinal bleeding in patients with known liver disease or portal vein thrombosis. Diagnostic modalities include:
* Capsule Endoscopy: Often the first-line investigation, providing direct visualization of the small bowel mucosa. however, it can be limited by poor visualization due to bleeding or capsule retention.
* Double-Balloon Enteroscopy (DBE): Allows for deeper enteroscopy and therapeutic intervention, including biopsy and potential variceal banding (though less common in SBV).
* Computed Tomography (CT) Angiography/magnetic resonance (MR) Angiography: Essential for identifying the venous anatomy, assessing the extent of varices, and evaluating for portal vein thrombosis or other vascular abnormalities. CT angiography and MR angiography are crucial for pre-procedural planning.
* Venography: The gold standard for confirming the diagnosis and mapping the venous anatomy prior to PTRE.
Percutaneous Transvenous Retrograde Embolization (PTRE) Technique
PTRE involves accessing the venous system, typically via the femoral vein, and navigating retrogradely to the superior mesenteric vein (SMV) and then to the variceal draining veins. Embolic agents, such as coils, sclerosants (e.g.,Onyx),or a combination,are then deployed to occlude the varices and reduce portal venous pressure.
The typical steps include:
- Venous Access & Catheterization: Establishing access, usually femoral, and advancing a catheter towards the SMV.
- Venography & Roadmapping: Detailed venography to visualize the variceal anatomy.
- selective Catheterization: Precise catheterization of the variceal draining veins.
- Embolization: Controlled deployment of embolic agents.
- Post-Embolization Assessment: Repeat venography to confirm complete occlusion and assess for complications.
Case Presentation: Adhesion-Related Complication
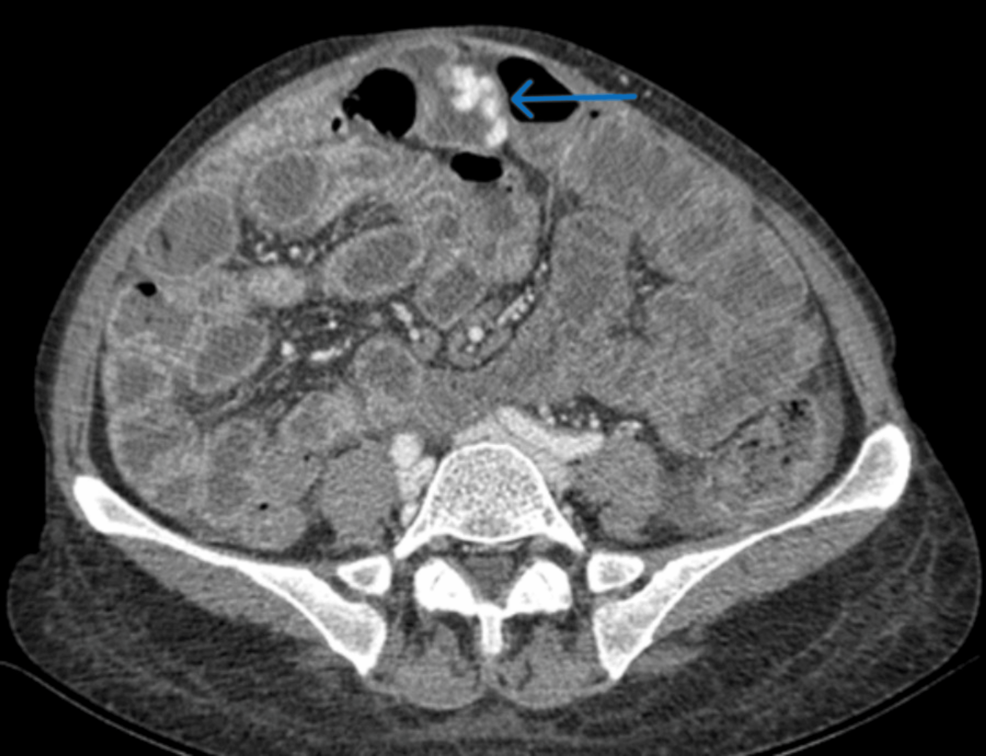
A 62-year-old male with cirrhosis secondary to chronic hepatitis C presented with recurrent episodes of melena and anemia. Capsule endoscopy revealed multiple SBV. CT angiography confirmed the diagnosis and demonstrated extensive varices draining into the SMV. PTRE was planned.
During the procedure, selective catheterization of a prominent variceal draining vein was achieved. Initial Onyx embolization was prosperous. Though, attempts to catheterize and embolize adjacent varices were hampered by significant resistance. Further venography revealed adhesion between the catheter tip and the intestinal wall, likely due to prior inflammation and variceal distortion.
This adhesion posed a significant risk of bowel perforation or injury. The procedure was temporarily halted. Gentle manipulation, combined with the use of a more flexible microcatheter, was employed to carefully dissect the adhesion. Once freed, successful embolization of the remaining varices was achieved. Bowel perforation is a rare but serious complication of PTRE.
Managing Adhesions during PTRE: Key Considerations
Adhesion formation is a recognized, though often underestimated, complication of PTRE in patients with SBV. several factors contribute to this:
* Chronic Inflammation: Underlying liver disease and variceal inflammation promote adhesion formation.
* Variceal Distortion: Large, distorted varices can physically adhere to surrounding structures.
* Catheter Trauma: Forceful catheter manipulation can exacerbate adhesion formation.
Strategies to mitigate adhesion-related complications include:
* Careful catheter Selection: Utilizing flexible microcatheters to minimize trauma.
* Gentle Manipulation: Avoiding forceful advancement of the catheter.
* Hydrophilic Catheters: Employing hydrophilic-coated catheters to reduce friction.
* Real-Time Imaging: Utilizing fluoroscopy and venography to carefully monitor catheter position and identify potential adhesions.
* **Consider