Discover the latest in health: evidence‑based wellness tips, medical breakthroughs, nutrition guidance, fitness insights, and expert advice for a healthier, happier life.
Anesthesiologists face unique challenges when providing care for patients with severe cavitary tuberculosis (TB) undergoing non-pulmonary surgery. The delicate balance between providing adequate anesthesia and minimizing the risk of barotrauma – lung injury caused by excessive pressure – is paramount. A recent case report highlights strategies for successfully managing anesthesia in such a complex scenario, offering valuable insights for clinicians.
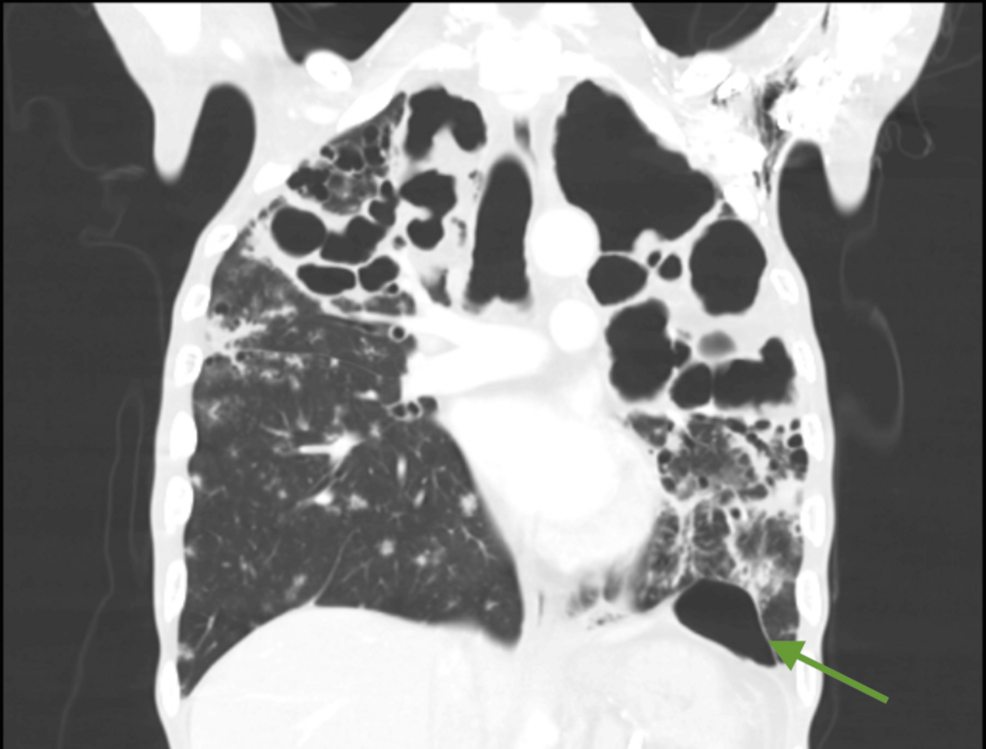
Cavitary tuberculosis, a severe form of the disease, leaves significant structural damage to the lungs, increasing vulnerability to complications during procedures requiring mechanical ventilation. The primary concern is the potential for rupture of existing cavities or the formation of new ones due to positive pressure ventilation. This case, involving abdominal surgery, underscores the need for meticulous planning and a tailored anesthetic approach to safeguard patients with this pre-existing lung condition.
The case report details a patient with extensive cavitary lesions undergoing abdominal surgery. The anesthesiology team employed a strategy centered around lung protection. This included careful titration of tidal volumes – the amount of air delivered with each breath – to minimize peak airway pressures. According to research on the effects of statins, beyond their lipid-lowering properties, they may offer some protective benefits in inflammatory conditions like HIV, which can similarly contribute to cardiovascular disease; however, this is not directly applicable to TB management but highlights the broader consideration of inflammation in vulnerable patients. Frontiers research suggests statins can modulate inflammatory responses.
Central to the anesthetic plan was the use of neuromuscular blocking agents to achieve complete muscle relaxation, allowing for better control of ventilation and reducing the perform of breathing. The team also utilized advanced monitoring techniques, including continuous assessment of airway pressures, oxygen saturation, and end-tidal carbon dioxide levels. These parameters provided real-time feedback, enabling prompt adjustments to the ventilation strategy. The choice of anesthetic agents was carefully considered, favoring those with minimal effects on lung function and cardiovascular stability.
The case also highlights the importance of understanding the potential interactions between anesthetic drugs and the patient’s underlying medical conditions. For example, research indicates that the HIV drug abacavir may be associated with an elevated risk of cardiovascular disease according to the National Institutes of Health. While not directly related to TB, this underscores the need for a comprehensive review of a patient’s medication list before surgery.
Inflammation plays a significant role in the progression of both HIV and cardiovascular disease, as noted by the New England Journal of Medicine and American Heart Association Journals. This systemic inflammation can exacerbate lung injury and increase the risk of complications during anesthesia.
The successful management of this case demonstrates the feasibility of performing abdominal surgery in patients with severe cavitary TB. However, it emphasizes the critical importance of a multidisciplinary approach, involving pulmonologists, surgeons, and anesthesiologists, to optimize patient outcomes. Careful patient selection, meticulous preoperative assessment, and a tailored anesthetic plan are essential components of this strategy.
Looking ahead, further research is needed to refine anesthetic protocols for patients with advanced TB. Studies investigating the optimal ventilation strategies, the role of novel monitoring techniques, and the potential benefits of adjunctive therapies could further improve the safety and efficacy of anesthesia in this vulnerable population. Continued vigilance and a commitment to individualized patient care will remain paramount in managing these complex cases.
Have you encountered similar challenges in managing anesthesia for patients with complex pulmonary conditions? Share your experiences and insights in the comments below.
Disclaimer: This information is intended for general knowledge and informational purposes only, and does not constitute medical advice. It is essential to consult with a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.