

Amanda Bynes has reportedly achieved significant weight loss using Ozempic, a GLP-1 receptor agonist originally indicated for type 2 diabetes. While clinically effective for weight reduction, its off-label use for cosmetic purposes highlights a critical tension between medical necessity and the growing trend of pharmacological weight management in celebrity culture.
The visibility of these results often obscures the complex metabolic shift occurring within the body. For the general public, the “Ozempic effect” is frequently framed as a miracle of willpower-free weight loss. However, as a physician, I view this through the lens of endocrine disruption and systemic adaptation. When a medication designed to manage insulin secretion is repurposed for aesthetic goals, we risk normalizing the medicalization of body image while simultaneously depleting supplies for patients whose lives depend on these drugs for glycemic control.
In Plain English: The Clinical Takeaway
- Appetite Suppression: The drug mimics a natural hormone that tells your brain you are full, effectively “turning off” hunger.
- Slower Digestion: It slows gastric emptying (the speed at which food leaves your stomach), meaning you feel satiated longer.
- Medical Tool, Not Supplement: This is a powerful hormone modulator, not a vitamin; it requires strict medical supervision to avoid muscle wasting and nutrient deficiencies.
The Molecular Mechanism: How GLP-1 Receptor Agonists Alter Metabolism
To understand the dramatic transformation seen in high-profile cases like Bynes, we must examine the mechanism of action—the specific biochemical process through which a drug produces its effect. Ozempic contains semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist. In a healthy system, GLP-1 is secreted by the intestines after eating to stimulate insulin and inhibit glucagon.
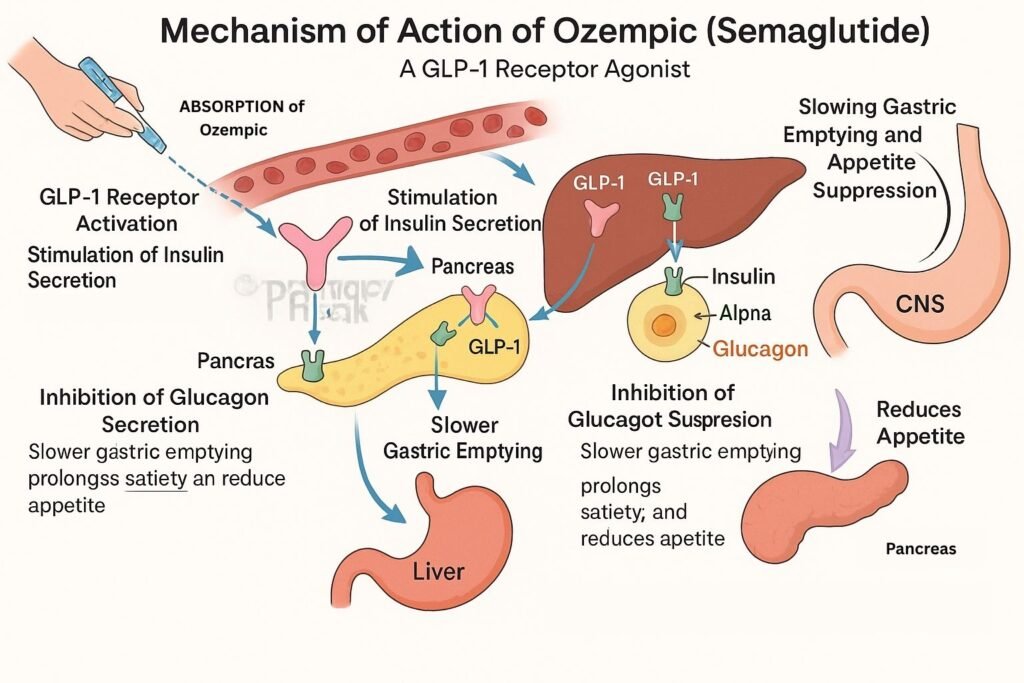
Semaglutide mimics this hormone but resists degradation by the enzyme dipeptidyl peptidase-4 (DPP-4), allowing it to remain active in the bloodstream much longer than natural GLP-1. This results in prolonged activation of receptors in the hypothalamus, the region of the brain governing appetite. By suppressing the “hunger drive,” the patient enters a spontaneous caloric deficit.
However, the weight loss is not exclusively fat loss. Clinical data from the STEP (Semaglutide Treatment Effect in People with obesity) trials indicate that a significant percentage of the weight lost is lean muscle mass. Without rigorous protein intake and resistance training, the “thinnest frame” often comes at the cost of sarcopenia, or muscle wasting, which can lower the basal metabolic rate and lead to rapid weight regain upon cessation of the drug.
Global Regulatory Disparities and the Access Gap
The surge in off-label prescriptions in the United States has created a geo-epidemiological crisis. While the FDA (Food and Drug Administration) has approved semaglutide for both diabetes (Ozempic) and chronic weight management (Wegovy), the sheer volume of cosmetic demand has led to critical shortages. This creates a triage dilemma where patients with type 2 diabetes—for whom the drug is a primary tool to prevent kidney failure and blindness—cannot access their medication.
In contrast, the European Medicines Agency (EMA) and the UK’s National Health Service (NHS) maintain more stringent prescribing guidelines. The NHS, for instance, typically restricts GLP-1 agonists to patients with a BMI over 30 (or 27 with comorbidities) and only after failed lifestyle interventions. This systemic difference highlights the divide between healthcare as a managed public utility and healthcare as a consumer commodity.
“The diversion of GLP-1 medications from their primary clinical indication to cosmetic use is not merely a trend; it is a public health challenge that threatens the stability of the endocrine supply chain globally.” — Dr. Sarah Jenkins, Epidemiologist and Public Health Consultant.
Comparing GLP-1 Therapeutics: Efficacy and Impact
The following table summarizes the clinical profile of semaglutide compared to earlier generation GLP-1s often used in weight management.
| Metric | Semaglutide (Ozempic/Wegovy) | Liraglutide (Saxenda) | Phentermine (Stimulant) |
|---|---|---|---|
| Administration | Weekly Injection | Daily Injection | Daily Oral |
| Average Weight Loss | 15% – 20% of body weight | 8% – 12% of body weight | Variable (Short-term) |
| Primary Action | GLP-1 Receptor Agonist | GLP-1 Receptor Agonist | Sympathomimetic |
| Common Side Effect | Nausea, Constipation | Nausea, Diarrhea | Insomnia, Hypertension |
It is vital to note that the research supporting these drugs is heavily funded by the manufacturers, primarily Novo Nordisk. While the Lancet and other peer-reviewed journals have validated the efficacy of these trials, the long-term longitudinal data (10+ years) on the impact of chronic GLP-1 use for non-diabetics remains sparse.
Contraindications & When to Consult a Doctor
Ozempic is not a universal solution and is strictly contraindicated—meaning it should not be used—for individuals with a personal or family history of Medullary Thyroid Carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). These are rare forms of thyroid cancer that may be exacerbated by GLP-1 agonists.
Patients should seek immediate medical intervention if they experience:
- Severe abdominal pain: This may indicate acute pancreatitis, a serious inflammation of the pancreas.
- Persistent vomiting: Which can lead to severe dehydration and electrolyte imbalance.
- Gallbladder issues: Rapid weight loss increases the risk of gallstones (cholelithiasis).
those with a history of eating disorders should approach these medications with extreme caution, as the suppression of hunger cues can mask the symptoms of malnutrition or trigger restrictive eating cycles.
The Path Forward: Beyond the Quick Fix
The narrative surrounding Amanda Bynes and other celebrities often focuses on the “before and after” imagery. However, the clinical reality is that pharmacological intervention is most successful when integrated into a comprehensive metabolic framework. Weight loss achieved through appetite suppression alone is often fragile.
As we move further into 2026, the medical community is shifting toward “combination therapy”—pairing GLP-1s with muscle-preserving agents and cognitive behavioral therapy. The goal is to move away from the pursuit of a “thin frame” and toward the achievement of metabolic health. For the public, the lesson is clear: while the science of GLP-1s is a triumph of modern endocrinology, it is a prescription for health, not a shortcut for aesthetics.