
Global icon Celine Dion announced her return to the stage this week, following a years-long hiatus due to a diagnosis of Stiff-Person Syndrome (SPS). The 58-year-ancient singer revealed plans for a series of concerts in Paris beginning in September, signaling a positive shift in her health journey. This news offers hope to the estimated 1 in 1 million individuals worldwide affected by this rare neurological disorder.
Dion’s public battle with SPS has brought much-needed attention to a condition often misdiagnosed or dismissed as psychological. Although the exact cause remains elusive, SPS is believed to be an autoimmune disorder impacting the central nervous system, leading to progressive muscle rigidity and debilitating spasms. Her willingness to share her experience is not only deeply personal but also serves as a crucial catalyst for increased research funding and improved patient care. The implications extend beyond celebrity news; it highlights the challenges faced by individuals living with rare neurological conditions and the importance of early diagnosis and multidisciplinary treatment approaches.
In Plain English: The Clinical Takeaway
- What is SPS? It’s a rare condition where your muscles become very stiff and you have painful spasms. It’s not caused by a problem with your nerves, but by your immune system attacking them.
- Can it be treated? There’s no cure, but treatments can aid manage the stiffness and pain, allowing people to live more comfortably and, in some cases, return to activities like performing.
- Why is Celine Dion’s case important? Her openness is raising awareness about this little-known condition, which can lead to faster diagnosis and better support for others.
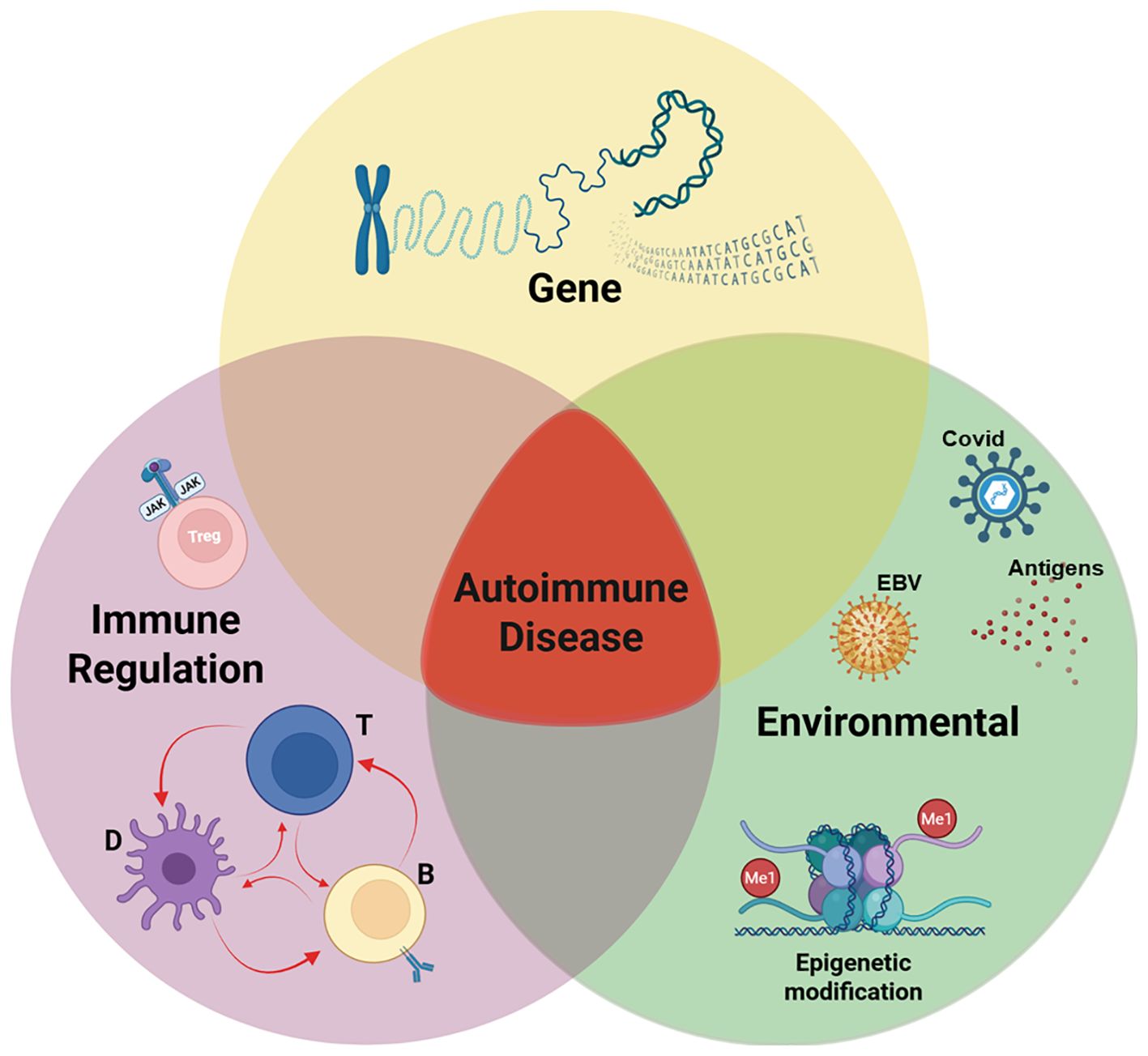
Understanding the Autoimmune Cascade in Stiff-Person Syndrome
Stiff-Person Syndrome (SPS) is classified as a neurological disorder characterized by fluctuating muscle rigidity and painful spasms. The pathophysiology is complex, but current research points to an autoimmune etiology. Specifically, elevated levels of antibodies targeting glutamic acid decarboxylase (GAD65) – an enzyme crucial for producing gamma-aminobutyric acid (GABA), an inhibitory neurotransmitter – are found in approximately 60-80% of SPS patients. Reduced GABAergic inhibition in the spinal cord and brainstem is thought to be the primary mechanism driving the hyper-excitability and subsequent muscle rigidity. But, a significant proportion of SPS cases (20-40%) are seronegative for GAD65 antibodies, suggesting other autoimmune targets are involved. Research is ongoing to identify these additional antigens.
The clinical presentation of SPS varies significantly. Some individuals experience gradual onset of stiffness primarily affecting the trunk and abdomen, while others present with more acute and severe spasms triggered by external stimuli like noise, touch, or emotional distress. The disease can significantly impair mobility, leading to falls and an increased risk of injury. Diagnosis is often delayed due to the rarity of the condition and the overlap with other neurological disorders. Electromyography (EMG) – a diagnostic test measuring electrical activity in muscles – can reveal continuous muscle activity even at rest, a hallmark of SPS.
The Role of Immunotherapies and Symptomatic Management
Currently, there is no cure for SPS. Treatment focuses on managing symptoms and improving quality of life. Immunotherapies, such as intravenous immunoglobulin (IVIg) and plasma exchange (PLEX), are often employed to modulate the immune system and reduce antibody levels. IVIg involves administering concentrated antibodies from healthy donors, while PLEX removes harmful antibodies from the patient’s blood. These treatments have demonstrated varying degrees of efficacy in clinical trials, with some patients experiencing significant symptom relief. However, the response to immunotherapy is often unpredictable, and long-term treatment may be required.
Symptomatic management includes the use of muscle relaxants (e.g., benzodiazepines, baclofen) to reduce muscle spasms and pain. Physical therapy and occupational therapy can help maintain mobility and functional independence. Psychological support is also crucial, as the chronic nature of SPS and its impact on daily life can lead to anxiety and depression. Recent research is exploring the potential of novel therapies, including monoclonal antibodies targeting specific immune cells involved in the autoimmune response.
| Treatment Modality | Mechanism of Action | Reported Efficacy | Common Side Effects |
|---|---|---|---|
| Intravenous Immunoglobulin (IVIg) | Modulates immune system; reduces autoantibody levels | 30-70% symptom reduction in responders | Headache, fatigue, infusion-related reactions |
| Plasma Exchange (PLEX) | Removes autoantibodies from circulation | Short-term symptom relief in some patients | Hypotension, infection risk, catheter-related complications |
| Baclofen | GABAB receptor agonist; reduces muscle spasticity | Variable; often used in combination with other therapies | Drowsiness, dizziness, nausea |
Geographical Impact and Access to Specialized Care
The prevalence of SPS is estimated to be 1-2 per million people, making it a rare disease globally. However, regional variations in diagnosis and reporting may exist. In Europe, access to specialized neurological care and immunotherapies varies significantly between countries. The European Medicines Agency (EMA) plays a crucial role in regulating the approval and availability of treatments for rare diseases like SPS. The EMA’s orphan drug designation incentivizes pharmaceutical companies to develop therapies for rare conditions. In the United States, the Food and Drug Administration (FDA) also offers similar incentives. However, even with regulatory approval, access to these therapies can be limited by cost and insurance coverage.

The establishment of specialized SPS clinics and centers of excellence is essential to improve diagnosis, treatment, and research. These centers can provide multidisciplinary care, including neurologists, immunologists, physical therapists, and psychologists. Increased awareness among healthcare professionals is also critical to reduce diagnostic delays and ensure timely access to appropriate treatment.
“The challenge with rare diseases like SPS is not just developing effective therapies, but also ensuring that patients have equitable access to those therapies, regardless of their geographic location or socioeconomic status.” – Dr. Maria Garcia, Neurologist, National Institute of Neurological Disorders and Stroke (NINDS)
Funding and Bias Transparency
Research on SPS is often hampered by limited funding due to its rarity. A significant portion of the research on autoimmune neurological disorders, including SPS, is funded by non-profit organizations like the National Organization for Rare Disorders (NORD) and patient advocacy groups. Pharmaceutical companies also contribute to research, particularly in the development of latest immunotherapies. It’s important to note that industry-funded research may be subject to potential bias, and researchers are obligated to disclose any conflicts of interest. NORD provides a comprehensive database of rare disease research funding opportunities and resources for patients and families.
Contraindications & When to Consult a Doctor
While immunotherapies like IVIg and PLEX are generally well-tolerated, they are not without risks. IVIg can cause allergic reactions, kidney problems, and blood clots. PLEX carries risks of hypotension, infection, and catheter-related complications. Individuals with a history of allergic reactions to blood products or kidney disease should discuss these risks with their doctor before undergoing IVIg or PLEX. Anyone experiencing unexplained muscle stiffness, painful spasms, or difficulty walking should consult a neurologist for evaluation. Early diagnosis and treatment are crucial to prevent disease progression and improve quality of life.
Celine Dion’s courageous announcement and return to the stage represent a beacon of hope for individuals living with SPS. Her story underscores the importance of continued research, improved access to care, and increased awareness of this challenging neurological condition. The future trajectory of SPS treatment hinges on identifying novel therapeutic targets and developing more effective and personalized treatment strategies.
References
- Dalakas MC, et al. “Stiff-person syndrome: pathophysiology, diagnosis, and treatment.” The Lancet Neurology 11.7 (2012): 639-647.
- Martinez-Martin P, et al. “Stiff-person syndrome revisited: an update on diagnosis, pathophysiology, and treatment.” Journal of Neurology, Neurosurgery & Psychiatry 88.1 (2017): 28-36.
- Schulz-Schüpke S, et al. “Clinical features and diagnostic criteria for stiff-person syndrome.” Neurology 68.16 (2007): 1386-1392.
- https://www.ninds.nih.gov/health-information/disorders/stiff-person-syndrome