
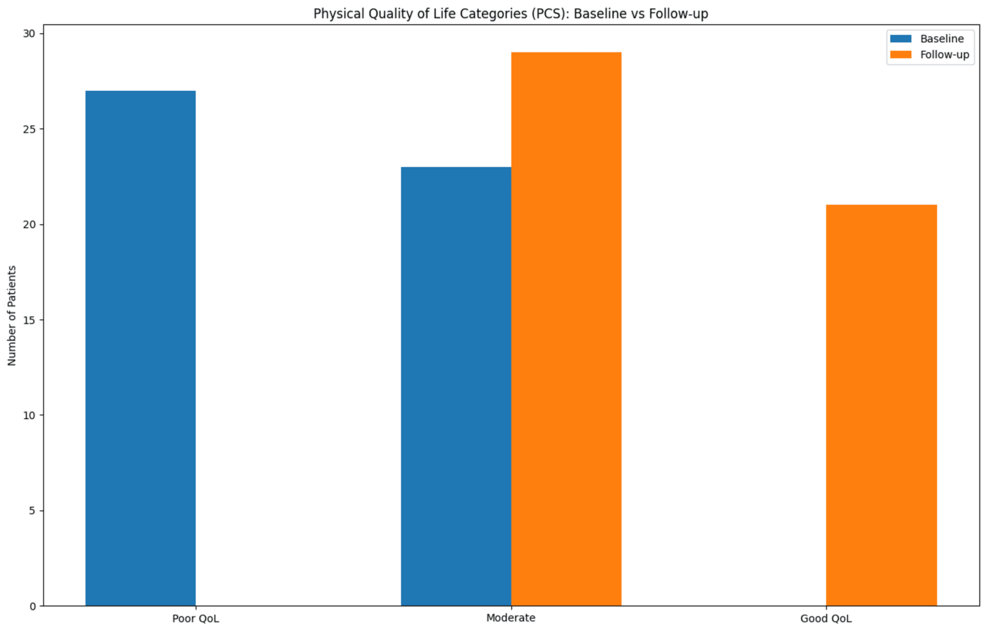
New research published in this week’s journal, Cureus, demonstrates that conservative management of early-stage hemorrhoids—utilizing dietary fiber, hydration, and lifestyle modifications—significantly improves patient Quality of Life (QoL) beyond simple symptom relief, reducing the immediate need for surgical intervention in a substantial portion of the adult population.
For too long, the medical community has viewed hemorrhoids as a mere nuisance or a localized physical ailment. Yet, the psychological burden—ranging from social anxiety to chronic discomfort—often goes undocumented in clinical settings. By shifting the focus from “stopping the bleed” to “holistic recovery,” this study underscores a critical paradigm shift in proctology: prioritizing non-invasive recovery to avoid the systemic risks and recovery downtime associated with surgical excision.
In Plain English: The Clinical Takeaway
- Fiber is a Tool, Not a Suggestion: Increasing soluble fiber doesn’t just “help”; it changes the physical consistency of stool to prevent the strain that causes blood vessels to swell.
- Conservative Management: This refers to treating the condition through diet, hydration, and topical agents rather than using surgery or invasive procedures.
- QoL Recovery: Success is measured not just by the absence of pain, but by the patient’s ability to return to normal daily activities and mental well-being.
The Pathophysiology of Vascular Cushions and the Role of Fiber
To understand why conservative management works, one must understand the mechanism of action—the specific biological process—of the hemorrhoidal plexus. Hemorrhoids are not merely “varicose veins” of the rectum; they are displaced vascular cushions composed of connective tissue, smooth muscle, and arteriovenous anastomoses (connections between arteries and veins) that aid in fecal continence.
When these cushions are subjected to chronic intra-abdominal pressure—the pressure inside the belly during straining—the supporting connective tissue weakens, and the cushions prolapse (slide out of place). Conservative management targets the root cause: the stool consistency.
Soluble fiber, such as psyllium husk, works by absorbing water to create a gel-like consistency. This reduces the friction against the anal mucosa (the lining of the rectum) and decreases the time and effort required for evacuation. By lowering the pressure on the hemorrhoidal plexus, the inflammation subsides, allowing the vascular cushions to return to a less congested state without the need for surgical trauma.
Global Standards: From the NHS to the ASCRS
The approach to hemorrhoidal care varies significantly across global healthcare systems. In the United Kingdom, the National Health Service (NHS) typically enforces a strict “conservative-first” triage pathway. Patients are encouraged to manage Grade I and II hemorrhoids (those that do not prolapse or those that retract spontaneously) through lifestyle changes before being referred to a consultant.
In contrast, the United States healthcare landscape, guided by the American Society of Colon and Rectal Surgeons (ASCRS), offers a broader spectrum of early interventions. While ASCRS guidelines also emphasize fiber and fluids, there is a higher prevalence of early adoption of office-based procedures like rubber band ligation (cutting off blood supply to the hemorrhoid). The Cureus study reinforces the NHS model, suggesting that for early-stage patients, the psychological and physical recovery found in conservative management is often equivalent to more aggressive interventions, but with zero surgical risk.
“The shift toward Patient-Reported Outcome Measures (PROMs) is essential. We are finding that the subjective recovery of a patient’s quality of life often outweighs the objective ‘disappearance’ of the hemorrhoid on a clinical exam.”
Comparative Efficacy: Conservative vs. Surgical Intervention
The decision to move from conservative management to surgery is usually based on the “Grade” of the hemorrhoid. The following table summarizes the clinical trajectory for early-stage management.
| Management Strategy | Target Grade | Primary Mechanism | Recovery Time | Primary Risk |
|---|---|---|---|---|
| Conservative | Grade I & II | Stool softening / Inflammation reduction | Immediate / Ongoing | Treatment non-compliance |
| Band Ligation | Grade II & III | Ischemic necrosis (cutting off blood) | 1–2 Weeks | Localized infection / Pain |
| Hemorrhoidectomy | Grade III & IV | Surgical excision of tissue | 4–8 Weeks | Anal stenosis (narrowing) |
Funding Transparency and the Open-Access Model
This research was published in Cureus, a PubMed-indexed, open-access journal. Unlike studies funded by pharmaceutical companies producing topical steroid creams or medical device manufacturers selling ligation kits, this specific research emphasizes lifestyle and dietary interventions. The absence of industry funding reduces the likelihood of “publication bias,” where only positive results for a specific drug are reported. The study’s reliance on patient-reported data ensures that the “Quality of Life” metric is the primary driver of the conclusion, rather than a corporate KPI.
Contraindications & When to Consult a Doctor
While conservative management is highly effective for early-stage hemorrhoids, it is not a universal cure. There are critical contraindications—situations where this approach is insufficient or dangerous.
You must seek immediate professional medical intervention if you experience:
- Unexplained Rectal Bleeding: While hemorrhoids cause bleeding, blood in the stool can also be a primary symptom of colorectal cancer or Inflammatory Bowel Disease (IBD). A digital rectal exam or colonoscopy is required to rule out malignancy.
- Severe Anemia: If chronic bleeding leads to fatigue, shortness of breath, or pallor, conservative management is no longer sufficient; blood transfusion or surgical ligation may be necessary.
- Grade IV Prolapse: When hemorrhoids are permanently prolapsed and cannot be pushed back in, dietary fiber will not “shrink” the tissue back into place; surgical intervention is typically required.
- Thrombosed Hemorrhoids: A blood clot within the hemorrhoid can cause acute, excruciating pain that requires an incision and drainage by a physician.
The Future of Proctological Recovery
The trajectory of hemorrhoid treatment is moving away from the scalpel and toward behavioral science. By validating the “Quality of Life” recovery associated with conservative management, clinicians can now provide patients with evidence-based confidence that they can manage their condition without the fear of the operating room. The goal is no longer just the removal of a physical protrusion, but the restoration of a patient’s dignity and daily comfort through sustainable, evidence-based lifestyle integration.