
A recent case report from Tanzania highlights a rare manifestation of disseminated tuberculosis (TB) in a newly diagnosed HIV-positive patient, presenting as a nodo-colonic fistula. This underscores the critical require for early HIV screening in TB patients to prevent severe, atypical opportunistic infections in immunocompromised populations.
This case is not merely a medical curiosity; it is a stark reminder of the synergistic devastation caused by the TB/HIV co-infection. When the immune system is compromised by HIV, tuberculosis ceases to be a localized pulmonary disease and becomes a systemic predator. For patients globally, In other words that “classic” symptoms—like a persistent cough—may be absent, replaced by atypical presentations that can mislead clinicians and delay life-saving intervention.
In Plain English: The Clinical Takeaway
- HIV changes the “map” of TB: In healthy people, TB usually stays in the lungs. In HIV-positive patients, it can travel through the blood to any organ, including the gut and lymph nodes.
- Atypical signs are red flags: A “fistula” (an abnormal tunnel between two organs) in the abdomen can be a sign of advanced, untreated TB in immunocompromised individuals.
- Concurrent treatment is vital: Treating TB without addressing HIV—or vice versa—is often insufficient. Both must be managed simultaneously to prevent relapse and death.
The Pathophysiology of Disseminated TB and Nodo-Colonic Fistulae
To understand this case, we must examine the mechanism of action—the specific biological process—by which Mycobacterium tuberculosis behaves in an HIV-positive environment. In a robust immune system, the body sequesters TB bacteria within “granulomas,” which are essentially biological prisons made of immune cells that keep the infection localized.

However, HIV targets and destroys CD4+ T-lymphocytes, the very cells required to maintain these granulomas. When the granuloma collapses, the bacteria escape into the bloodstream, leading to disseminated tuberculosis (TB that has spread from the original site to other organs). In the Tanzanian case, the bacteria migrated to the mesenteric lymph nodes and the wall of the colon.
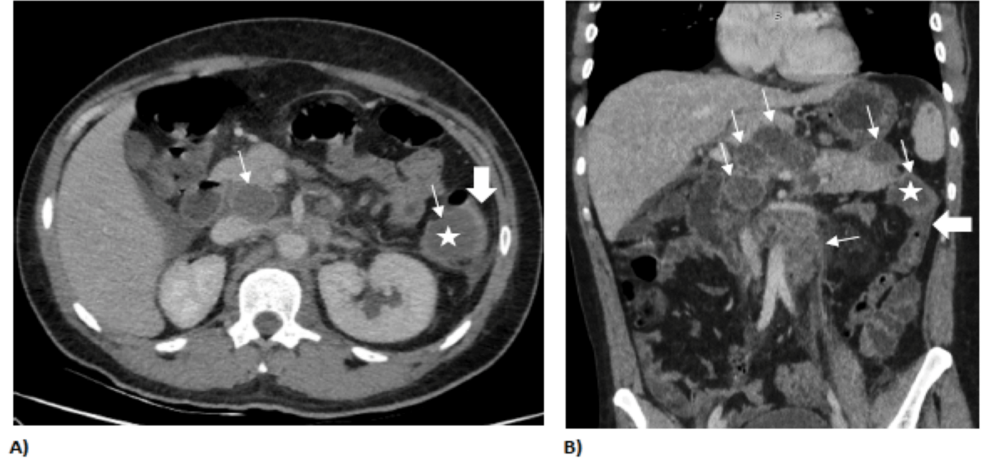
The result was a nodo-colonic fistula: a pathological communication or “tunnel” that formed between an infected lymph node and the lumen of the colon. This occurs because the inflammatory response causes tissue necrosis (cell death), creating a hole that allows intestinal contents to leak into the lymph node or vice versa, leading to severe abdominal pain and systemic sepsis.
The Global Syndemic: Geo-Epidemiological Bridging
While this case originated in Tanzania, the clinical implications resonate from the clinics of Dar es Salaam to the wards of the NHS in the UK and the CDC-monitored sites in the US. We are dealing with a “syndemic”—two epidemics interacting to worsen the outcome of both. According to the World Health Organization (WHO), TB remains the leading cause of death for people living with HIV globally.
In Sub-Saharan Africa, the challenge is often diagnostic access. The “gold standard” for TB diagnosis, the GeneXpert MTB/RIF assay, allows for rapid detection, but its availability varies. In contrast, in high-income regions like the US or EU, clinicians may overlook disseminated TB because it is rarer, leading to “diagnostic blindness” where the patient is treated for Crohn’s disease or colon cancer instead of an opportunistic infection.
“The intersection of HIV and Tuberculosis is one of the most challenging frontiers in global health. We are not just fighting two pathogens; we are fighting the collapse of the host’s cellular defense architecture.” — Dr. Rama Chandra, Epidemiologist specializing in Infectious Diseases.
Comparing Clinical Presentations: Pulmonary vs. Disseminated TB
The following table delineates the divergence in clinical presentation between standard TB and the disseminated form seen in HIV-positive patients.
| Clinical Feature | Pulmonary TB (Typical) | Disseminated TB (HIV-Positive) |
|---|---|---|
| Primary Site | Lungs (Apical segments) | Multi-organ (Liver, Spleen, Bone Marrow, Gut) |
| Chest X-Ray | Clear cavitary lesions | Often normal or non-specific infiltrates |
| Sputum Culture | Usually positive (High bacterial load) | Frequently negative (Paucibacillary) |
| Common Complication | Hemoptysis (Coughing blood) | Organ failure, Fistulae, Meningitis |
| Diagnostic Urgency | High | Critical (High risk of rapid sepsis) |
Funding, Bias, and the Open-Access Model
This case report was published in Cureus, a PubMed-indexed, open-access journal. Case reports are typically funded by the authors’ home institutions or through individual practitioner contributions. There are no pharmaceutical conflicts of interest reported in this instance, as the treatment followed standard WHO-recommended first-line anti-TB therapy (Rifampicin, Isoniazid, Pyrazinamide, and Ethambutol) and Antiretroviral Therapy (ART).
However, the reliance on case reports highlights a gap in large-scale longitudinal data for atypical TB presentations in East Africa. Most funding is directed toward pulmonary TB, leaving “extrapulmonary” (outside the lungs) TB under-researched and under-funded.
Contraindications & When to Consult a Doctor
Treatment for TB/HIV co-infection is complex. Contraindications—reasons why a specific treatment should not be used—often arise during the administration of Rifampicin, which can have severe interactions with certain ART drugs (specifically some protease inhibitors), potentially reducing the efficacy of HIV medication.
patients must be monitored for Immune Reconstitution Inflammatory Syndrome (IRIS). This occurs when the immune system recovers so rapidly after starting ART that it “overreacts” to the remaining TB antigens, causing a paradoxical worsening of symptoms. What we have is not a failure of treatment, but a dangerous immune surge that requires steroids rather than more antibiotics.
Seek immediate medical attention if you experience:
- Unexplained weight loss exceeding 10% of body mass in three months.
- Drenching night sweats and persistent low-grade fever.
- Severe abdominal pain accompanied by changes in bowel habits or blood in the stool.
- A persistent cough that does not respond to standard antibiotics.
The Path Forward: Integrated Screening
The Tanzanian case serves as a clinical mandate: we must move toward integrated “one-stop” screening. Every patient presenting with TB must be tested for HIV, and every HIV-positive patient must be screened for latent TB. The transition from a pulmonary infection to a nodo-colonic fistula is a journey of systemic failure that can be halted with early detection and the aggressive application of evidence-based protocols.