
Recent clinical evaluations from Oxford University confirm that Cognitive Behavioral Therapy (CBT) significantly reduces the frequency and intensity of panic attacks. By retraining the brain to reinterpret physical sensations, this evidence-based psychological intervention offers a sustainable alternative or adjunct to pharmacotherapy for patients suffering from panic disorder.
For millions globally, a panic attack is not merely “stress”—This proves a systemic failure of the body’s alarm system. The findings emerging this week emphasize a critical shift in psychiatric care: moving away from the temporary suppression of symptoms via medication toward the permanent restructuring of the patient’s cognitive response. While benzodiazepines may halt a panic attack in progress, they do not teach the patient why the attack happened or how to prevent the next one. CBT fills this gap by targeting the cognitive distortions that fuel the cycle of panic.
In Plain English: The Clinical Takeaway
- Retraining the Brain: CBT teaches you that the “suffocating” feeling of a panic attack is a harmless physical glitch, not a medical emergency.
- Long-Term Stability: Unlike some medications that only work while you take them, CBT provides a “toolkit” of skills that reduce the likelihood of relapse.
- Facing the Fear: The treatment involves safely triggering mild physical symptoms to prove to your brain that you are not in actual danger.
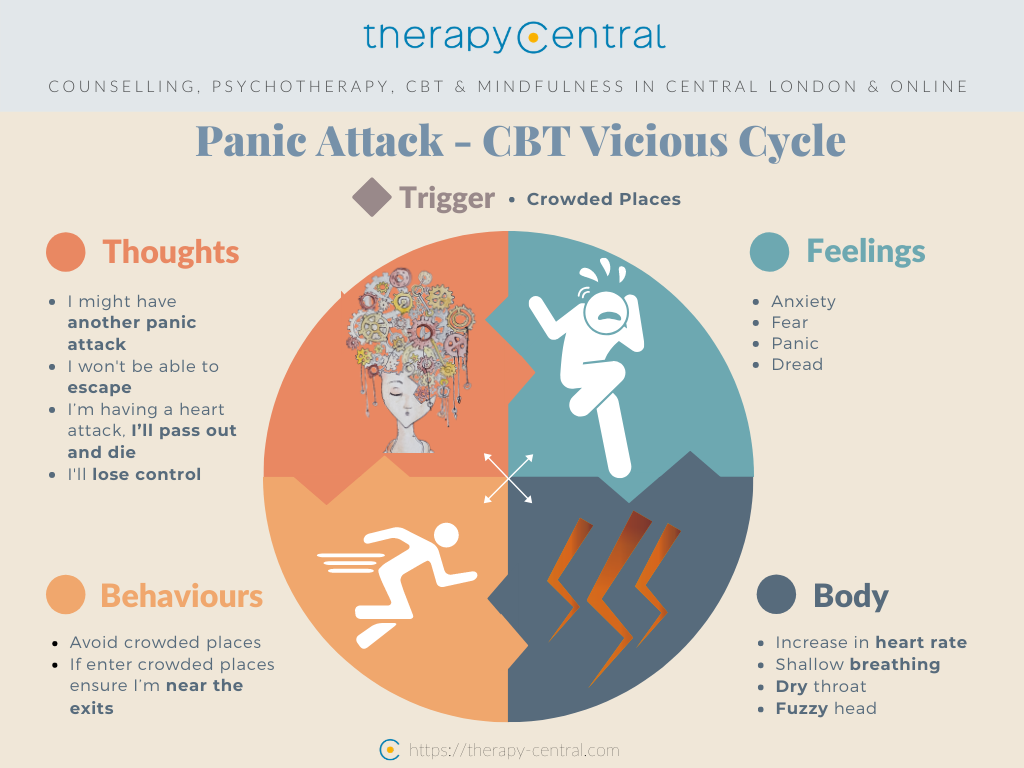
The Mechanism of Action: Breaking the Catastrophic Loop
To understand why CBT is effective, we must examine its mechanism of action—the specific biological and psychological process through which a treatment produces its effect. Panic disorder is driven by “catastrophic misinterpretation.” This occurs when a patient experiences a normal somatic sensation (such as a slightly elevated heart rate) and incorrectly labels it as a sign of imminent death or insanity.
Professor David Clark’s research at Oxford focuses on interoceptive exposure. This is a clinical technique where patients are encouraged to deliberately induce the physical sensations they fear—such as spinning in a chair to create dizziness or breathing through a straw to simulate shortness of breath. By repeatedly experiencing these sensations in a controlled environment without a negative outcome, the amygdala (the brain’s fear center) undergoes a process of extinction learning. The brain eventually stops triggering the “fight-or-flight” response to these internal cues.
This process is far more rigorous than general “talk therapy.” It is a structured, goal-oriented protocol that leverages the brain’s neuroplasticity to decouple the physical sensation from the psychological panic response. According to data indexed in PubMed, this approach significantly lowers the baseline anxiety levels of patients compared to those receiving supportive therapy alone.
Comparative Efficacy: CBT vs. Pharmacological Intervention
The clinical debate often centers on whether psychotherapy or medication is superior. In reality, the choice depends on the patient’s specific pathology and the desired duration of effect. While Selective Serotonin Reuptake Inhibitors (SSRIs) are effective at modulating serotonin levels to stabilize mood, they often carry a side-effect profile that includes weight gain or sexual dysfunction.
The following table summarizes the clinical distinctions between the primary treatment modalities for panic disorder:
| Treatment Modality | Primary Mechanism | Onset of Action | Relapse Risk | Common Side Effects |
|---|---|---|---|---|
| CBT | Cognitive Restructuring / Extinction Learning | Gradual (8-16 weeks) | Low (Skill-based) | Temporary increase in anxiety |
| SSRIs | Serotonin Reuptake Inhibition | Moderate (2-6 weeks) | Moderate (Post-discontinuation) | Nausea, Insomnia, Weight gain |
| Benzodiazepines | GABAergic Enhancement (CNS Depression) | Rapid (30-60 mins) | High (Dependency risk) | Sedation, Cognitive impairment |
The Oxford study’s use of a randomized controlled trial (RCT)—the gold standard of clinical research where patients are randomly assigned to a treatment or control group to eliminate bias—demonstrates that CBT’s efficacy is not merely a placebo effect. The durability of CBT is particularly noteworthy. patients who complete a full course of CBT often maintain their gains years later, whereas medication-only patients frequently relapse upon cessation of the drug.
Global Access and Regulatory Frameworks
The translation of this research into public health policy varies by region. In the United Kingdom, the National Health Service (NHS) has integrated CBT into its “Improving Access to Psychological Therapies” (IAPT) program, making it a first-line treatment. This systemic integration reduces the financial barrier to entry for patients who might otherwise rely on cheaper, but potentially addictive, sedative medications.
In the United States, the FDA does not “approve” therapy in the way it approves drugs, but the American Psychological Association (APA) recognizes CBT as an evidence-based practice. However, access remains fragmented due to insurance disparities. In East Asia, including South Korea, there is a growing movement to shift from a purely pharmacological model to one that incorporates structured psychotherapy, though the stigma surrounding mental health continues to be a barrier to early intervention.
“The goal of treating panic is not to eliminate the possibility of a panic attack, but to eliminate the fear of the attack. Once the fear is gone, the attacks naturally cease to occur.”
This perspective, echoed by leading clinical psychologists in the field of anxiety disorders, highlights the difference between symptom management and actual recovery. The research conducted by the Oxford team was largely supported by university grants and public health funding, reducing the risk of corporate bias often found in pharmaceutical-sponsored trials.
Contraindications & When to Consult a Doctor
While CBT is highly effective, it is not a universal solution. It is contraindicated—meaning it may not be appropriate or could be harmful—for individuals in the midst of an acute psychotic episode or those with severe, untreated Major Depressive Disorder (MDD) where the patient lacks the cognitive energy to engage in exposure exercises.
You should seek immediate professional medical intervention if:
- Physical Mimicry: You have not had a cardiovascular screening to rule out arrhythmias or pulmonary issues that can mimic panic attacks.
- Suicidal Ideation: You are experiencing thoughts of self-harm, as CBT for panic must be secondary to crisis stabilization.
- Severe Agoraphobia: Your fear of leaving the house is so profound that you cannot attend therapy sessions, necessitating a combination of home-based care and medication to “prime” the patient for CBT.
The Future of Panic Disorder Treatment
As we glance toward the future of psychiatric care, the integration of digital health—such as VR-based exposure therapy—is likely to expand the reach of the Oxford model. By simulating the environments that trigger panic in a controlled, virtual setting, clinicians can accelerate the extinction learning process.
The evidence is clear: panic disorder is a treatable condition. Through the rigorous application of Cognitive Behavioral Therapy, patients can move from a state of constant hyper-vigilance to one of cognitive mastery. The shift from “treating a symptom” to “training a brain” represents the most significant advancement in public mental health intelligence this decade.
References
- The Lancet – Psychiatry and Mental Health Archives
- World Health Organization (WHO) – Mental Health Gap Action Programme (mhGAP)
- Centers for Disease Control and Prevention (CDC) – Mental Health Surveillance
- Oxford University Department of Psychiatry – Clinical Trial Database on Anxiety Disorders