
As the 2026 midterm elections approach, healthcare policy has transcended political debate to turn into a primary determinant of public health. Current analysis indicates that voter concerns regarding cost and access directly correlate with morbidity rates in chronic conditions like diabetes and hypertension. This brief examines the clinical implications of the 2026 electoral landscape.
In my dual capacity as a practicing physician and a medical journalist, I observe a critical convergence: the ballot box is becoming a prescription pad. The upcoming 2026 midterms are not merely about fiscal allocation; they are about the structural integrity of the American healthcare safety net. When voters prioritize healthcare costs, they are indirectly voting on their own life expectancy and quality of life. The data suggests that policy stagnation is now a measurable risk factor for preventable disease progression.
In Plain English: The Clinical Takeaway
- Policy as Prevention: Legislative decisions on drug pricing and insurance coverage act as “upstream” preventative medicine, determining whether patients can afford the treatments that keep them out of the hospital.
- The Adherence Gap: High out-of-pocket costs lead to “medication non-adherence,” where patients skip doses of critical drugs like insulin or antihypertensives, increasing the risk of stroke and heart failure.
- Mental Health Infrastructure: Election outcomes will dictate funding for mental health parity laws, directly impacting access to therapy and psychiatric medication for millions of Americans.
The Pathophysiology of Financial Toxicity
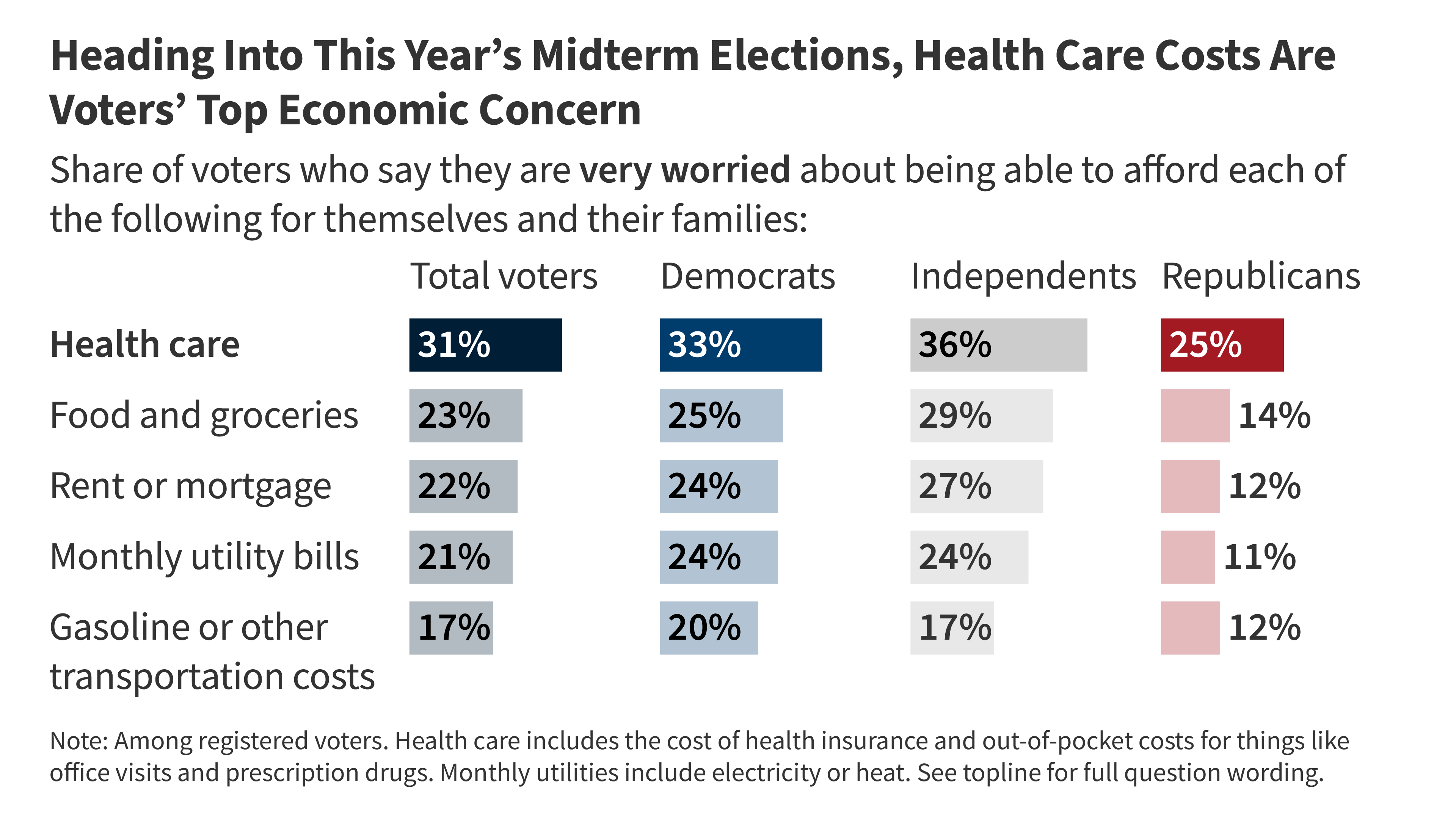
The KFF issue brief highlights that the cost of care remains a top economic concern for voters. From a clinical perspective, we classify this as financial toxicity. This is not a metaphor; it is a physiological stressor. When patients face high deductibles or copayments, the body’s stress response activates, elevating cortisol levels which can exacerbate cardiovascular issues. More critically, financial toxicity leads to the rationing of care.

In 2026, we are seeing a disturbing trend where patients delay seeking care for early-stage symptoms due to cost fears. This delay shifts the clinical presentation from manageable acute conditions to complex, chronic emergencies. For example, a patient avoiding a primary care visit for persistent chest pain due to cost concerns may eventually present at the Emergency Department with an acute myocardial infarction. The electoral focus on cost containment is, a focus on reducing emergency room overcrowding and improving long-term survival rates.
“Social determinants of health, including economic stability and access to care, account for up to 50% of health outcomes. When policy fails to address affordability, we are effectively prescribing poor health to our most vulnerable populations.” — Dr. Vivek Murthy, U.S. Surgeon General (Contextualized for 2026 Policy Frameworks)
Geo-Epidemiological Bridging: The US vs. Global Standards
To understand the stakes of the 2026 election, we must look beyond domestic borders. In the United Kingdom, the National Health Service (NHS) operates on a model where access is decoupled from employment status. In the European Union, the EMA (European Medicines Agency) facilitates faster cross-border access to novel therapies. In contrast, the US system remains fragmented.
The 2026 electoral debate centers on whether the US will move toward a model that prioritizes population health metrics over fee-for-service revenue. If the current trajectory of high out-of-pocket costs continues, we risk widening the gap between US health outcomes and those of peer nations. Specifically, maternal mortality rates and management of Type 2 diabetes remain areas where US policy lags behind global averages, despite higher per-capita spending. The election serves as a referendum on whether the US healthcare system will prioritize equity of access.
Funding Transparency and Bias Analysis
It is crucial to note the funding sources behind the data driving this election cycle. The KFF (Kaiser Family Foundation), cited in the initial brief, is a non-partisan source of information on national health issues. Still, pharmaceutical lobbying groups and insurance conglomerates heavily fund opposing political action committees (PACs). This creates a conflict of interest landscape where policy may favor shareholder returns over patient outcomes. As medical journalists, we must scrutinize legislation that lowers drug prices for the government while potentially stifling R&D for orphan diseases, ensuring a balanced view of innovation vs. Accessibility.
The following table summarizes the projected clinical impact of varying policy stances likely to be debated in the 2026 midterms:
| Policy Focus Area | Clinical Mechanism of Impact | Potential Patient Outcome (2026-2030) |
|---|---|---|
| Drug Price Negotiation | Increases medication adherence by lowering copays for chronic conditions (e.g., insulin, statins). | Reduced hospitalization rates for diabetic ketoacidosis and cardiovascular events. |
| Medicaid Expansion | Expands the insured pool, allowing for earlier detection of cancers and infectious diseases. | Shift in cancer diagnosis from Stage IV (metastatic) to Stage I/II (localized), improving 5-year survival. |
| Mental Health Parity | Mandates insurance coverage for behavioral health equal to physical health. | Decrease in suicide rates and substance use disorder overdoses; improved management of comorbidities. |
Contraindications & When to Consult a Doctor
While political engagement is vital for public health, it is not a substitute for immediate medical care. Patients should not delay treatment while waiting for election outcomes or policy changes.

- Do Not Ration Medication: If you are struggling to afford prescriptions, consult your physician immediately. There are often patient assistance programs, generic alternatives, or therapeutic substitutes available that do not require waiting for legislative action.
- Emergency Symptoms: Chest pain, sudden onset of severe headache, difficulty breathing, or signs of stroke (FAST: Face drooping, Arm weakness, Speech difficulty, Time to call 911) require immediate emergency intervention regardless of insurance status. Under the EMTALA Act, emergency stabilizing treatment cannot be denied.
- Mental Health Crisis: If you or someone you know is experiencing a mental health crisis, do not wait for policy reforms. Contact the 988 Suicide & Crisis Lifeline immediately.
The Future Trajectory of Care
The 2026 election will likely define the healthcare architecture for the next decade. The shift from reactive care (treating sickness) to proactive care (maintaining wellness) depends entirely on the regulatory environment established by the incoming administration and Congress. As we analyze the polling data, voters understand this connection intuitively. The challenge for the medical community is to ensure that the resulting policies are grounded in epidemiological evidence rather than ideological rhetoric. The health of the nation depends on a system that values clinical efficacy and patient access above all else.
References
- KFF (Kaiser Family Foundation). “Health Care in the 2026 Elections: Issue Brief.”
- Centers for Disease Control and Prevention. “Social Determinants of Health: Know What Affects Health.”
- The New England Journal of Medicine. “Financial Toxicity and Cancer Treatment.”
- World Health Organization. “Monitoring Health for the SDGs: Sustainable Development Goals.”
- Office of the Surgeon General. “Social Connection and Health Framework.”