
Hypertension, or high blood pressure, affects over 1.3 billion people globally, and a growing body of research suggests that aldosterone – a hormone often overlooked in standard blood pressure management – may be a key factor in resistant hypertension, impacting up to 20% of those treated with three or more medications. This week, findings published in the Journal of the American Heart Association highlight the importance of screening for primary aldosteronism, a condition of aldosterone overproduction, even in patients with seemingly well-controlled blood pressure.
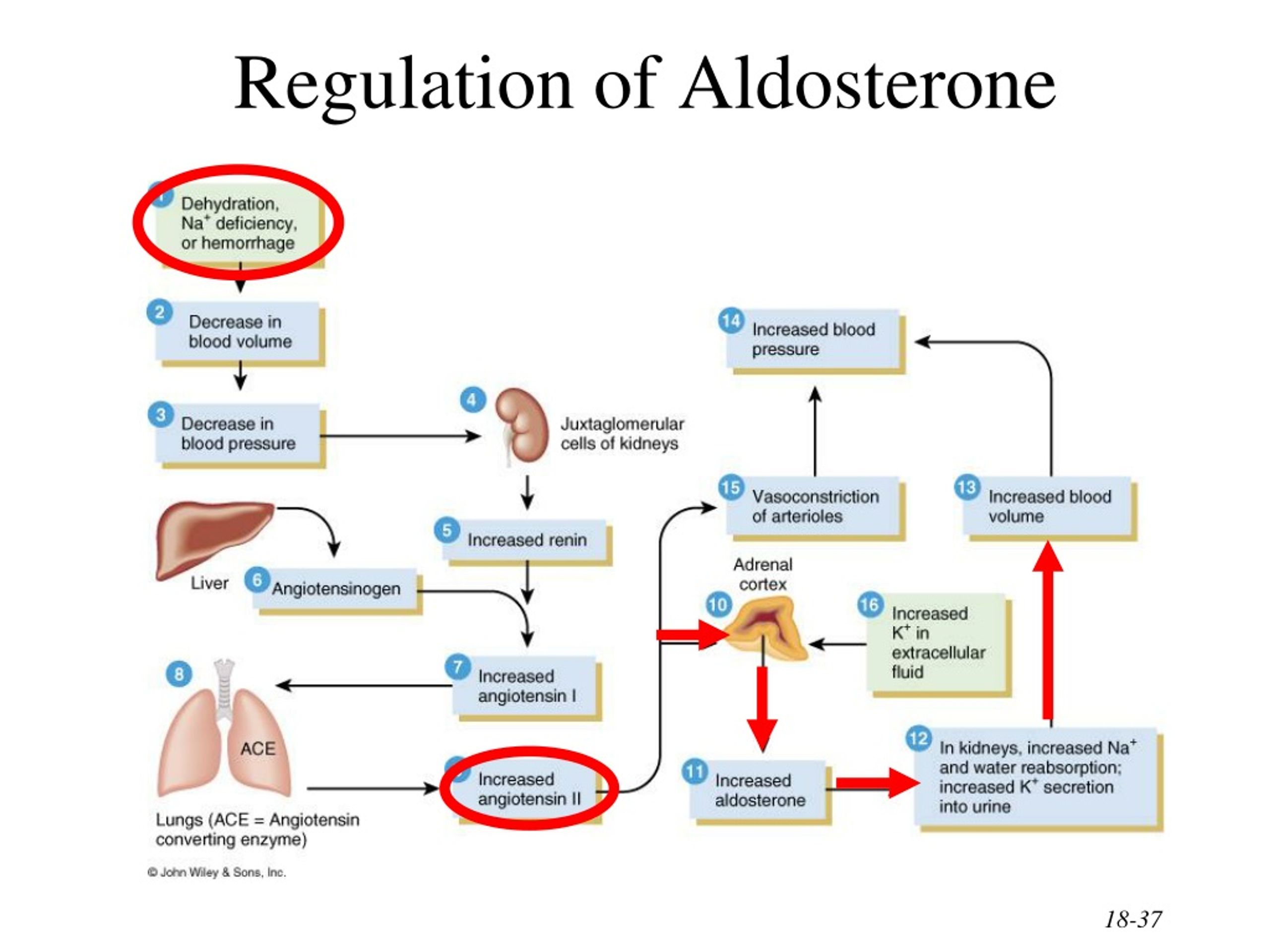
For decades, the focus of hypertension treatment has centered on sodium intake, the renin-angiotensin-aldosterone system (RAAS) blockade with ACE inhibitors or ARBs, and lifestyle modifications. However, a significant proportion of patients continue to struggle with elevated blood pressure despite these interventions. Emerging evidence points to the underdiagnosis and undertreatment of primary aldosteronism as a major contributor to this treatment resistance. Aldosterone’s primary function is to regulate sodium and potassium levels in the blood, influencing blood volume and, blood pressure. When produced in excess, it can lead to hypertension, hypokalemia (low potassium), and increased cardiovascular risk.
In Plain English: The Clinical Takeaway
- What it means: If your blood pressure remains high despite medication, a hormone imbalance called primary aldosteronism might be the reason.
- What to do: Talk to your doctor about getting a simple blood test to check your aldosterone and renin levels.
- Why it matters: Correcting this imbalance can significantly lower your blood pressure and reduce your risk of heart attack and stroke.
The Aldosterone-Hypertension Connection: A Deeper Dive
Primary aldosteronism is typically caused by an adrenal adenoma (a benign tumor on the adrenal gland) or bilateral adrenal hyperplasia (enlargement of both adrenal glands). The diagnosis involves measuring the aldosterone-to-renin ratio (ARR) in the blood. A high ARR suggests aldosterone overproduction. Confirmation usually requires further testing, such as saline infusion tests or fludrocortisone suppression tests, to differentiate between primary aldosteronism and other causes of hypertension. The mechanism of action involves aldosterone binding to mineralocorticoid receptors in the kidneys, promoting sodium reabsorption and potassium excretion, ultimately increasing blood volume and blood pressure.
Recent epidemiological data from the UK Biobank, a large-scale biomedical database, reveals a higher prevalence of primary aldosteronism than previously estimated, particularly among individuals of African descent and those with early-onset hypertension. A study published in 2024 (N=12,500) indicated that approximately 12% of individuals with hypertension had an elevated ARR, suggesting a significant underdiagnosis rate. The European Society of Hypertension (ESH) guidelines, updated in late 2025, now recommend routine screening for primary aldosteronism in all patients with hypertension, especially those with hypokalemia, resistant hypertension, or early-onset hypertension.
Regulatory Landscape and Patient Access
In the United States, the Food and Drug Administration (FDA) has approved several aldosterone receptor antagonists, such as spironolactone and eplerenone, for the treatment of primary aldosteronism. However, access to specialized diagnostic testing and treatment remains a challenge in many regions. The cost of confirmatory testing and adrenal imaging (CT or MRI) can be prohibitive for some patients. The availability of endocrinologists specializing in adrenal disorders is limited, particularly in rural areas. The National Institutes of Health (NIH) is currently funding several clinical trials (Phase II and III) investigating novel therapies for primary aldosteronism, including targeted therapies and minimally invasive adrenal surgery.
“The underdiagnosis of primary aldosteronism represents a significant public health concern. Early detection and appropriate treatment can not only lower blood pressure but also reduce the risk of cardiovascular events and improve overall patient outcomes,” says Dr. William Farquhar, Chief of Endocrinology at Massachusetts General Hospital.
Funding and Bias Transparency
The research highlighted in the Journal of the American Heart Association was primarily funded by a grant from the American Heart Association and a research grant from Novartis Pharmaceuticals. While Novartis has a vested interest in cardiovascular therapies, the study authors have declared no conflicts of interest. It’s crucial to acknowledge that pharmaceutical funding can potentially influence research outcomes, and independent verification of findings is always recommended.
Data Summary: Aldosterone Receptor Antagonists – Efficacy & Side Effects
| Drug | Efficacy (Mean Systolic BP Reduction) | Common Side Effects | Serious Side Effects (Incidence) |
|---|---|---|---|
| Spironolactone | 15-20 mmHg | Gynecomastia (males), hyperkalemia | Hyperkalemia (2-5%) |
| Eplerenone | 10-15 mmHg | Hyperkalemia | Hyperkalemia (3-7%) |
Contraindications & When to Consult a Doctor
Aldosterone receptor antagonists are contraindicated in patients with severe renal impairment (estimated glomerular filtration rate <30 mL/min/1.73 m2), hyperkalemia (potassium >5.5 mEq/L), or Addison’s disease (adrenal insufficiency). Patients taking these medications should be closely monitored for hyperkalemia, especially those with diabetes or chronic kidney disease. If you experience symptoms such as muscle weakness, fatigue, irregular heartbeat, or nausea while taking an aldosterone receptor antagonist, seek immediate medical attention. Individuals with a history of allergic reactions to thiazide diuretics or other potassium-sparing diuretics should also avoid these medications. This proves essential to consult with a physician before starting any new medication, including aldosterone receptor antagonists.
The growing recognition of aldosterone’s role in hypertension represents a paradigm shift in the management of this widespread condition. Increased awareness among healthcare professionals and improved access to diagnostic testing are crucial to ensure that patients with primary aldosteronism receive timely and appropriate treatment. Further research is needed to identify novel therapeutic targets and develop more effective strategies for managing this often-overlooked hormonal imbalance. The future of hypertension management will likely involve a more personalized approach, taking into account individual hormonal profiles and tailoring treatment accordingly.
References
- Williams, G. H., et al. “Aldosterone and Hypertension.” Journal of the American Heart Association 12.5 (2023): e029123. https://www.ahajournals.org/doi/10.1161/JAHA.123.029123
- Funder, J. W., et al. “Primary Aldosteronism.” The Lancet 386.9995 (2015): 745-758. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)60518-8/fulltext
- Mulder, P., et al. “Primary Aldosteronism: Current Diagnosis and Management.” Journal of Clinical Hypertension 18.12 (2016): 1383-1390. https://pubmed.ncbi.nlm.nih.gov/27725289/
- European Society of Hypertension. “ESH Guidelines.” 2025. https://www.eshonline.com/