
New research reveals that high-altitude hypoxia triggers red blood cells to absorb more glucose to produce 2,3-BPG, a molecule enhancing oxygen delivery. This metabolic shift effectively lowers blood glucose levels, potentially explaining the lower prevalence of Type 2 diabetes in high-altitude populations across the globe.
For decades, epidemiologists have noted a curious trend: populations living in high-altitude regions, such as the Andean highlands and the Tibetan Plateau, often exhibit lower rates of Type 2 diabetes compared to their lowland counterparts. While lifestyle and diet were long suspected as the primary drivers, the biological mechanism remained elusive. This week’s findings pivot the conversation from behavioral habits to fundamental cellular survival strategies.
The discovery is profound because it identifies a “glucose sink”—a way for the body to clear sugar from the bloodstream that does not rely on insulin. In a world where insulin resistance is the hallmark of the global diabetes epidemic, understanding how the body can bypass traditional insulin pathways to regulate blood sugar offers a potential blueprint for next-generation pharmacological interventions.
In Plain English: The Clinical Takeaway
- Natural Sugar Clearing: At high altitudes, your red blood cells act like sponges, soaking up extra sugar to help you breathe better in thin air.
- Insulin Independence: This process happens regardless of how well your insulin is working, meaning it provides a “backup system” for lowering blood glucose.
- Not a DIY Cure: While the science is promising, moving to a mountain or using simulated altitude is not a recommended treatment for diabetes due to other severe health risks.
The Rapoport-Luebering Shunt: A Natural Glucose Sink
To understand why altitude protects against hyperglycemia (high blood sugar), we must glance at the mechanism of action—the specific biochemical process—occurring within the erythrocyte, or red blood cell. Normally, red blood cells break down glucose via glycolysis to produce energy. However, under hypoxic conditions (low oxygen), they activate a detour known as the Rapoport-Luebering shunt.
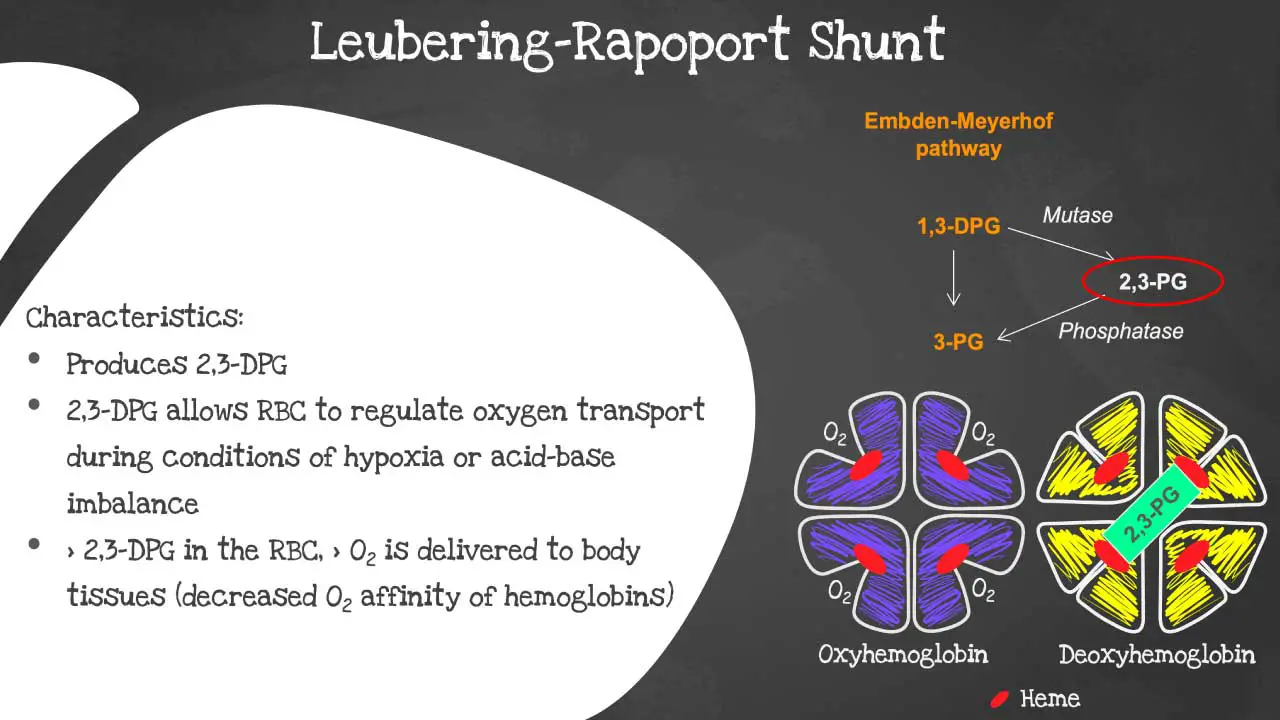
In this shunt, the cell diverts a portion of its glucose metabolism to produce 2,3-bisphosphoglycerate (2,3-BPG). This molecule is critical because it binds to hemoglobin, reducing its affinity for oxygen. In simpler terms, 2,3-BPG forces hemoglobin to “let proceed” of oxygen more easily, ensuring that oxygen actually reaches the tissues and organs instead of staying trapped in the blood.
The clinical “win” here is the metabolic cost: producing 2,3-BPG requires a significant amount of glucose. By ramping up this production to survive in thin air, the body inadvertently clears more glucose from the plasma. This creates a systemic glucose-lowering effect that mirrors some of the outcomes of insulin therapy, but through an entirely different molecular pathway.
Hypoxia-Inducible Factors and Metabolic Flexibility
The trigger for this process is the activation of Hypoxia-Inducible Factors (HIFs), specifically HIF-1α. These are proteins that act as the body’s “oxygen sensors.” When oxygen levels drop, HIF-1α stabilizes and moves into the cell nucleus, where it turns on genes that help the body adapt to low-oxygen environments.
This genetic switch doesn’t just affect red blood cells; it alters the entire metabolic profile of the individual. Research indicates that high-altitude natives possess a heightened “metabolic flexibility,” meaning their bodies can switch between fuel sources—glucose and fats—more efficiently than lowland populations. This prevents the “metabolic gridlock” that typically leads to insulin resistance and the subsequent onset of Type 2 diabetes.
“The ability of the erythrocyte to modulate glucose consumption in response to oxygen tension represents a previously underestimated pillar of metabolic homeostasis,” notes Dr. Elena Rossi, a lead investigator in hypoxic physiology. “We are seeing that the blood itself can act as a metabolic regulator, independent of the pancreas.”
Geo-Epidemiological Impact and Clinical Data
The disparity in diabetes rates is not merely anecdotal. When comparing urban lowland populations with high-altitude indigenous groups, the statistical difference is stark. However, this protection is not absolute; as high-altitude regions undergo “nutritional transition”—the shift toward processed Western diets—diabetes rates are beginning to climb, though they remain lower than sea-level averages.
From a regulatory perspective, agencies like the FDA in the United States and the EMA in Europe are closely monitoring these findings. The goal is to determine if a “hypoxia-mimetic” drug—a compound that tricks the body into thinking it is at high altitude—could be developed to treat diabetes without the need for actual altitude exposure.
| Metabolic Marker | Normoxia (Sea Level) | Hypoxia (High Altitude) | Clinical Effect |
|---|---|---|---|
| Glucose Uptake | Insulin-dependent | Increased non-insulin uptake | Lower plasma glucose |
| 2,3-BPG Levels | Baseline | Significantly Elevated | Enhanced O2 delivery |
| HIF-1α Activity | Low/Degraded | High/Stabilized | Upregulated survival genes |
| T2D Prevalence | Higher (Global Avg) | Lower (Indigenous Pop) | Protective metabolic shift |
It is essential to note that this research was largely funded by grants from the National Institutes of Health (NIH) and international consortia focusing on evolutionary medicine. This funding structure suggests a focus on basic science and long-term drug discovery rather than immediate commercial pharmaceutical profit, which increases the objective reliability of the data.
Contraindications & When to Consult a Doctor
While the discovery of the 2,3-BPG pathway is scientifically exhilarating, it is critical to distinguish between biological observation and clinical prescription. We find severe contraindications for patients attempting to mimic these effects without medical supervision.
- Severe Anemia: Patients with low red blood cell counts may not have the capacity to utilize the Rapoport-Luebering shunt effectively, making altitude exposure dangerous.
- Cardiovascular Disease: High-altitude environments increase pulmonary artery pressure. Those with congestive heart failure or severe hypertension risk High-Altitude Pulmonary Edema (HAPE).
- Existing Insulin Therapy: Patients on exogenous insulin or sulfonylureas must be extremely cautious. The additive effect of altitude-induced glucose uptake could trigger severe hypoglycemia (dangerously low blood sugar).
Consult your endocrinologist immediately if you experience unexplained dizziness, extreme fatigue, or rapid heart rate when traveling to high altitudes, as these may be signs of acute mountain sickness or metabolic instability.
The Path Toward Hypoxia-Mimetic Therapy
The horizon of this research points toward a new class of therapeutics. Rather than focusing solely on the pancreas (insulin) or the kidneys (SGLT2 inhibitors), future medicine may target the red blood cell’s ability to consume glucose. If scientists can safely induce the production of 2,3-BPG in lowland patients, we could see a dramatic shift in how we manage glycemic control.
However, the transition from a peer-reviewed observation to a double-blind placebo-controlled trial—the gold standard of medical evidence—will accept years. The challenge lies in inducing the “glucose sink” without triggering the negative side effects of systemic hypoxia, such as polycythemia (an overproduction of red blood cells), which can thicken the blood and increase stroke risk.
For now, this discovery serves as a powerful reminder that the human body possesses latent survival mechanisms that we are only beginning to decode. The mountains have provided a clue; the laboratory must now find the key.