
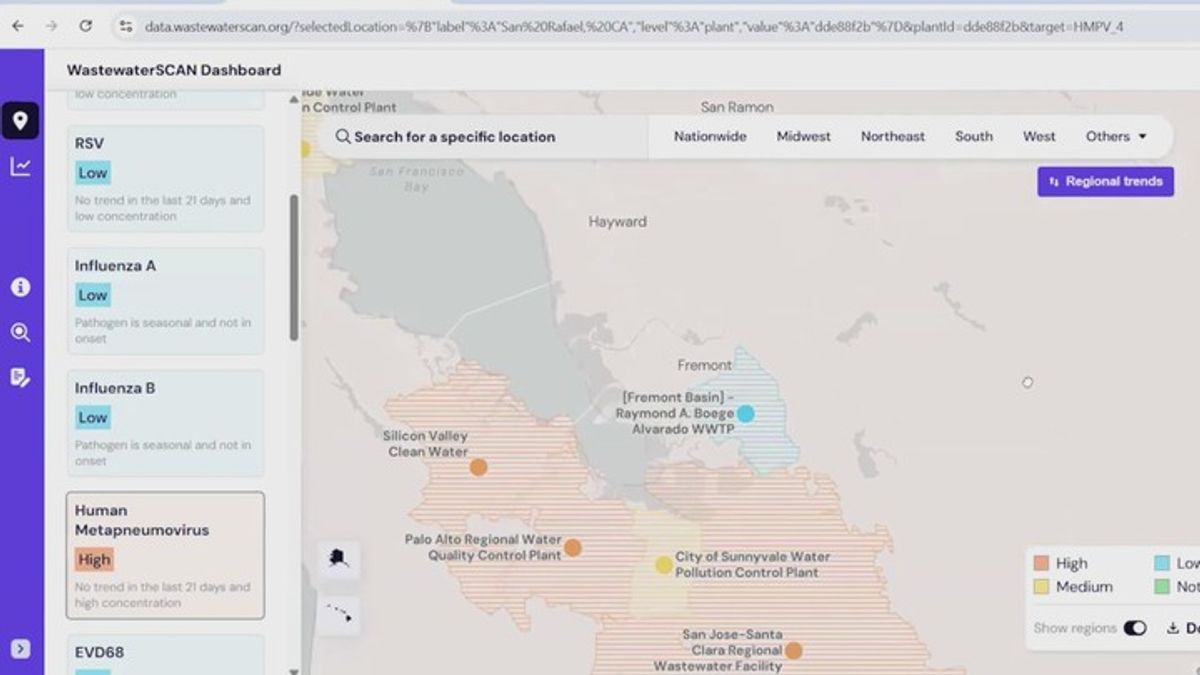
The San Francisco Bay Area is currently experiencing a surge in Human Metapneumovirus (HMPV) cases. This respiratory virus causes cold-like symptoms and pneumonia, primarily affecting infants, the elderly, and immunocompromised individuals. Public health officials are monitoring the spike to ensure regional hospital capacity remains stable during the spring season.
Although often overshadowed by Influenza or RSV, HMPV is a significant clinical entity that demands attention because it frequently presents as a “co-infection,” meaning a patient may be fighting two viruses simultaneously. For the general population, this may result in a lingering cough. still, for vulnerable populations, it can lead to severe lower respiratory tract infections that require hospitalization. Understanding the trajectory of this spike is critical for managing outpatient triage and reducing the burden on Bay Area emergency departments.
In Plain English: The Clinical Takeaway
- What it is: A common respiratory virus that looks like a cold but can turn into pneumonia in high-risk patients.
- Who is at risk: Young children, senior citizens, and people with weakened immune systems.
- What to do: Practice standard hygiene; most cases resolve with rest and hydration, but seek assist if breathing becomes difficult.
The Molecular Mechanism of HMPV Infection
Human metapneumovirus belongs to the Paramyxoviridae family. Its mechanism of action—the specific way it causes disease—involves the virus attaching to the respiratory epithelium (the lining of your airways) and utilizing the host cell’s machinery to replicate. This process triggers an inflammatory response, leading to the production of mucus and cellular debris that obstructs the narrow airways of infants.
Unlike the common cold, HMPV has a high affinity for the lower respiratory tract. This means it doesn’t just stay in the nose and throat; it can migrate deep into the lungs, causing bronchiolitis (inflammation of the small airways) or pneumonia. Because the symptoms mimic those of Respiratory Syncytial Virus (RSV), clinicians often require a multiplex PCR test—a highly sensitive molecular tool—to distinguish between the two.
Epidemiological Patterns and Regional Impact
The current spike in the Bay Area aligns with a broader global trend where HMPV peaks in late winter and early spring. However, the intensity of this year’s surge may be influenced by “immunity debt,” a phenomenon where populations have less natural exposure to common viruses due to previous social distancing and masking protocols, leaving the immune system less prepared for seasonal spikes.
In the United States, the Centers for Disease Control and Prevention (CDC) monitors these trends via the National Respiratory and Enteric Virus Network. The impact on the Bay Area is felt most acutely in pediatric clinics and long-term care facilities. When HMPV spikes, it places a secondary strain on the healthcare system, as patients who cannot breathe effectively require supplemental oxygen and nebulizer treatments.
“HMPV is often the ‘forgotten’ respiratory virus because it is so similar to RSV, but its ability to cause severe pneumonia in the elderly makes it a critical target for seasonal surveillance.” — Dr. Aris Thessaloniki, Epidemiologist and Viral Research Lead.
| Feature | Common Cold (Rhinovirus) | HMPV | RSV |
|---|---|---|---|
| Primary Site | Upper Respiratory | Upper & Lower Respiratory | Lower Respiratory (Infants) |
| Severity | Mild | Moderate to Severe | Severe in Neonates |
| Peak Season | Year-round | Late Winter/Spring | Winter |
| Treatment | Supportive Care | Supportive Care | Supportive/Prophylactic |
Funding, Bias, and the Search for a Vaccine
Currently, there is no FDA-approved vaccine or specific antiviral medication for HMPV. Treatment is purely supportive, meaning doctors treat the symptoms (fever, cough) rather than the virus itself. Most research into HMPV vaccines is funded by government grants through the National Institutes of Health (NIH) and various academic consortia, which reduces the likelihood of commercial bias in the reported efficacy of early-stage trials.
Ongoing research is focusing on mRNA-based delivery systems, similar to those used in COVID-19 vaccines. These trials aim to trigger the production of neutralizing antibodies that prevent the virus from entering the respiratory cells. However, most of these candidates are still in Phase I or II trials, meaning they are being tested for safety and dosage in small groups before moving to large-scale efficacy tests.
Geo-Epidemiological Bridging: US vs. Global Response
While the Bay Area is seeing a spike, the response differs globally. In the UK, the NHS integrates HMPV monitoring into its wider respiratory surveillance, often treating it as part of a broader “winter pressures” strategy. In the US, the decentralized nature of healthcare means that local departments, like those in San Francisco and Oakland, must coordinate to manage bed capacity.
The lack of a standardized, rapid-test kit available at all primary care offices in the US creates an “information gap.” Many patients are diagnosed with a “general respiratory infection” when they actually have HMPV. This lack of precise data can lead to the misuse of antibiotics, which are ineffective against viruses and contribute to the global crisis of antimicrobial resistance.
Contraindications & When to Consult a Doctor
Because HMPV is a virus, antibiotics are strictly contraindicated—they will not cure the infection and may cause unnecessary side effects like gastrointestinal distress. Patients should avoid self-medicating with strong cough suppressants in infants, as coughing is a necessary mechanism to clear mucus from the lungs.
Seek immediate medical attention if you or your child experience:
- Dyspnea: Shortness of breath or labored breathing (noticeable pulling in of the chest muscles).
- Cyanosis: A bluish tint to the lips or fingernails, indicating low oxygen saturation.
- High-Grade Fever: A fever that does not respond to acetaminophen or ibuprofen.
- Altered Mental State: Extreme lethargy or inability to wake an infant.
As we move further into the spring of 2026, the trajectory of HMPV will likely follow its natural seasonal decline. However, this spike serves as a reminder that our respiratory health is an ecosystem. Vigilance in hygiene and the continued pursuit of a targeted vaccine remain our best defenses against the “hidden” viruses that challenge our public health infrastructure.