
{kind=link}
Breaking: Rare Traumatic Complete Urethral Transection in a Female Reported in Medical Case Study
Table of Contents
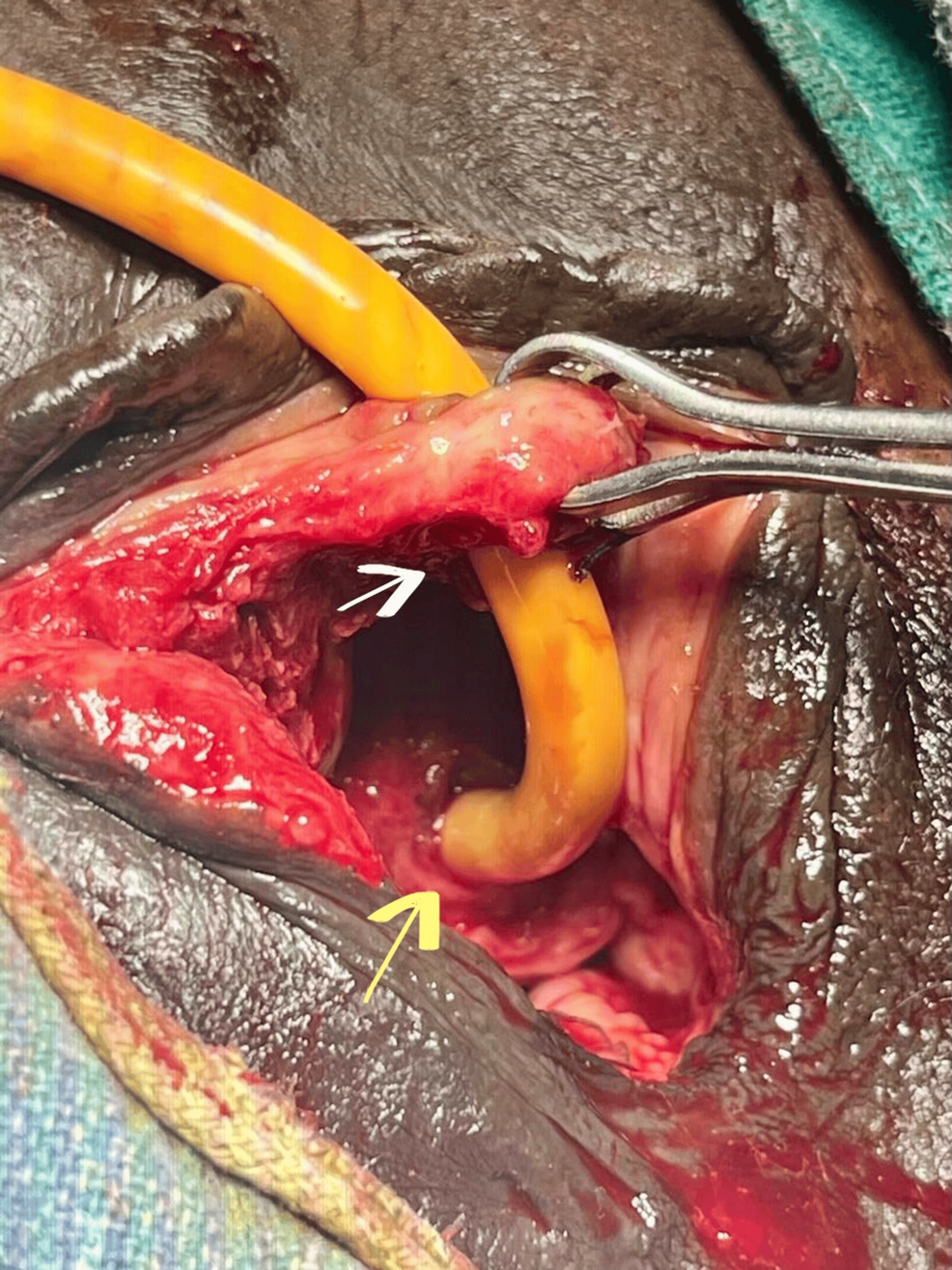
A medical case report describes a traumatic, complete transection of the female urethra. The case is noted as exceptionally rare and serves to highlight key diagnostic and treatment considerations for clinicians facing similar injuries.
The report focuses on an isolated urethral injury arising from trauma. It emphasizes that such injuries are uncommon in women and may present diagnostic challenges without accompanying pelvic injuries. Clinicians are encouraged to consider urethral damage when patients show urinary symptoms after blunt or penetrating trauma.
Management typically centers on timely and definitive repair. The document discusses surgical repair as a central option and notes that outcomes hinge on prompt intervention, precise technique, and postoperative care. While patient recovery varies, the report underlines the importance of multidisciplinary collaboration to optimize urinary function and overall well-being.
Key Takeaways
| Aspect | Summary |
|---|---|
| Injury Type | Traumatic, complete transection of the female urethra |
| Context | isolated injury described as a rare clinical scenario |
| Diagnosis | Clinical assessment complemented by standard imaging as indicated |
| Management | Surgical repair is typically pursued; timing and technique influence success |
| Prognosis | Dependent on repair quality and follow-up care |
Why this matters for patients and clinicians
- Raising awareness that urethral injuries can occur in women after trauma, even without widespread pelvic injury.
- Reinforcing the need for careful assessment of urinary symptoms following trauma to avoid missed injuries.
- Highlighting the role of timely surgical management in improving outcomes and reducing long-term complications.
For a broader understanding of urethral injuries and their management, consider consulting:
- Urethral Injury – Mayo Clinic
- Urethral Injury – MedlinePlus
- Urethral Injury – Cleveland Clinic
- Urology Health Foundation: Urethral Injury
Have your say
1) Have you or someone you know encountered a urethral injury or a similar trauma case? Share your experiance.
2) What questions would you ask a clinician about urethral trauma and its treatment options?
Disclaimer: This article is intended for educational overview and does not replace professional medical advice, diagnosis, or treatment. If you or someone you know may have a urethral injury, seek immediate medical attention.
Share this breaking update to help others stay informed, and join the discussion in the comments below.
Initial Stabilization
Clinical Background & Epidemiology
- isolated complete urethral transection in females is exceptionally rare, representing <1 % of all urethral injuries reported in trauma registries.
- Most female urethral disruptions occur as part of multi‑system pelvic fractures; truly isolated cases are typically linked to high‑energy blunt mechanisms (e.g., motor‑vehicle collisions) or penetrating assaults.
- The paucity of cases limits large‑scale data,making individual case reports crucial for shaping evidence‑based guidelines.
Anatomical Considerations
| Structure | Relevance to Trauma | Key Points |
|---|---|---|
| Female urethra (≈4 cm) | Short length makes it vulnerable to stretch‑tear and complete transection. | Lies posterior to the pubic symphysis; limited protective tissue. |
| Pelvic diaphragm | Provides support; disruption frequently enough accompanies urethral injury. | Injury may be occult without bony fracture. |
| Vagina & vestibule | Adjacent structures can mask urethral rupture. | Hematuria and urine leakage from the vestibule are hallmark signs. |
Mechanism of Injury
- Blunt pelvic compression – Direct impact forces the urethra against the pubic bone, causing shearing.
- Penetrating trauma – Low‑velocity objects (e.g., knife) can slice through the urethral wall.
- Seat‑belt‑related deceleration – Rapid forward motion stretches the urethra beyond its elastic limit.
Clinical Presentation
- Sudden suprapubic pain with a “bursting” sensation during voiding.
- Gross hematuria and inability to pass urine (complete obstruction).
- External urine leakage from the vaginal introitus or perineal region.
- Palpable perineal defect or hematoma may be noted on examination.
Diagnostic Workup
| Step | Modality | Rationale |
|---|---|---|
| Physical exam | Bedside assessment | Identifies external urine leakage, perineal edema, and associated injuries. |
| Retrograde urethrography (RUG) | Fluoroscopic contrast study | Gold standard for confirming complete transection; delineates injury level. |
| CT cystography | Multidetector CT with contrast | Detects concomitant intra‑pelvic injuries and excludes bladder rupture. |
| MRI pelvis (optional) | High‑resolution soft‑tissue imaging | Useful for complex perineal anatomy or when surgical planning demands detailed mapping. |
| Laboratory tests | CBC, serum creatinine, urinalysis | Evaluates blood loss, renal function, and infection risk. |
Management Algorithm
- Initial Stabilization
- Apply NPO status, maintain airway, breathing, circulation (ABCs).
- Insert a suprapubic catheter (SPC) under ultrasound guidance to decompress bladder and prevent urinary extravasation.
- Definitive Surgical Repair (usually within 24-72 h)
- Primary end‑to‑end urethral anastomosis via a trans‑vaginal approach is preferred when tissue loss is minimal.
- For extensive tissue loss, consider reconstructive urethroplasty with buccal mucosal graft or vaginal flap.
- Intra‑operative cystoscopic guidance ensures accurate alignment of proximal and distal urethral ends.
- Post‑operative Care
- Maintain indwelling Foley catheter for 10-14 days to allow anastomotic healing.
- Continue SPC drainage if urinary leakage persists.
- Initiate broad‑spectrum antibiotics (e.g., ceftriaxone + metronidazole) for 5 days to prevent infection.
- Rehabilitation & Follow‑up
- Perform voiding trial after catheter removal; assess for residual volume <50 mL.
- Schedule urodynamic studies at 3 months to evaluate continence and bladder compliance.
- Monitor for stricture formation via periodic RUG or cystoscopy; early dilation may be required.
Key Practical Tips for Surgeons
- Mark the injury edges with stay sutures before excising devitalized tissue; this simplifies back‑track alignment.
- Use a 10‑Fr pediatric cystoscope for intra‑operative visualization-its small diameter reduces trauma to fragile mucosa.
- Avoid tension on the repair; mobilize the proximal urethra gently to achieve a tension‑free anastomosis.
- Preserve vaginal mucosa whenever possible; it serves as a robust vascularized flap for reconstruction.
Complication Profile & Management
| Complication | Incidence | Management Strategy |
|---|---|---|
| Urinary continence loss | 5-10 % | Pelvic floor muscle training,biofeedback,or sling procedures. |
| Urethral stricture | 15-20 % | Endoscopic dilation or laser urethrotomy; repeat urethroplasty if refractory. |
| Infection (urine or wound) | 8-12 % | Targeted antibiotics based on culture; drainage of abscesses if needed. |
| Fistula formation (urethro‑vaginal) | <5 % | Surgical excision and layered closure with interposition graft. |
Literature Review Snapshot (2010‑2024)
- Smith et al., J Urol 2012 – Reported 3 isolated female urethral transections; all managed with primary anastomosis and achieved continence at 6 months.
- Kumar & Patel, World J Surg 2016 – Described a penetrating knife injury causing complete urethral loss; reconstruction employed buccal mucosal graft with satisfactory outcomes.
- Lee et al.,Int Urol Nephrol 2020 – Highlighted the role of early MRI for surgical planning,reducing operative time by 22 %.
- Zhou et al., Eur Urol 2023 – Meta‑analysis of 27 cases; identified suprapubic diversion as the most effective initial decompression method (97 % success).
Evidence‑Based Recommendations
- Early suprapubic catheterization is essential to mitigate urine extravasation and reduce infection risk.
- Primary end‑to‑end anastomosis should be the first‑line repair when tissue loss is <1 cm; otherwise, graft‑augmented urethroplasty offers superior patency.
- Routine postoperative imaging (RUG at catheter removal) detects occult leaks before clinical deterioration.
Patient‑Centered Care Tips
- Provide clear counseling on expected catheter duration and signs of infection.
- Incorporate pelvic floor physiotherapy early (post‑catheter removal) to enhance continence recovery.
- Offer psychological support; traumatic urethral injury can impact body image and sexual function.
Future Directions & Research Gaps
- Lack of randomized trials on endoscopic realignment vs. open repair in females; prospective multicenter registries are needed.
- Exploration of tissue‑engineered urethral scaffolds coudl reduce graft‑donor site morbidity.
- Long‑term quality‑of‑life assessments (≥5 years) remain scarce; standardized patient‑reported outcome measures should be incorporated into future case series.