

In Kenya, approximately 92 newborns and 15 mothers die daily from preventable complications. These deaths primarily result from postpartum hemorrhage, sepsis, and neonatal asphyxia. This crisis is driven by systemic gaps in skilled birth attendance and inadequate postnatal care, highlighting a critical failure in the regional healthcare infrastructure.
This mortality rate is not merely a statistical tragedy; This proves a clinical failure of the “Three Delays” model: the delay in deciding to seek care, the delay in reaching a health facility, and the delay in receiving adequate care upon arrival. When a woman dies from a preventable cause, it indicates a breakdown in the continuum of care, from prenatal screening to the critical 48-hour postnatal window. For the global medical community, Kenya’s crisis serves as a stark reminder that medical innovation is useless if the delivery mechanism—the healthcare system—is fractured.
In Plain English: The Clinical Takeaway
- Most deaths are avoidable: The majority of these fatalities are caused by heavy bleeding or infections that can be treated with basic, low-cost medications.
- The “Golden Window”: The first 48 hours after birth are the most dangerous; receiving professional medical check-ups during this time drastically reduces death rates.
- Skilled Attendance: Giving birth in a clinic with a trained midwife, rather than at home without assistance, is the single most effective way to prevent newborn death.
The Physiology of Preventable Mortality: PPH and Sepsis
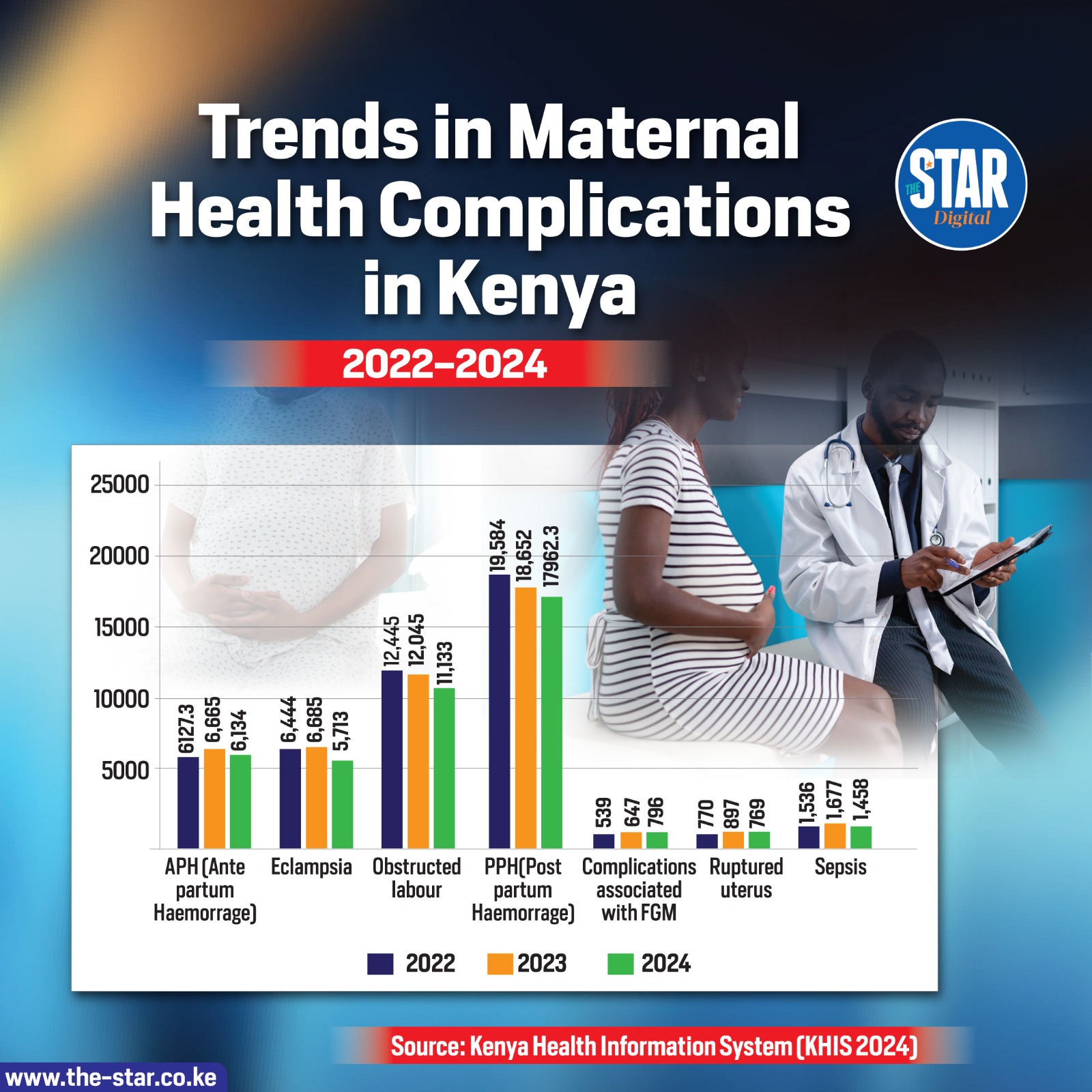
The primary driver of maternal death in Kenya is postpartum hemorrhage (PPH), defined as heavy bleeding after childbirth. The clinical mechanism of action here is often uterine atony—a condition where the uterine muscles fail to contract after the placenta is delivered. Without these contractions, the blood vessels at the placental site remain open, leading to rapid, catastrophic blood loss.
To combat this, the gold standard is the administration of uterotonics, such as oxytocin, which stimulate the uterus to contract. But, oxytocin requires a “cold chain” (refrigerated storage), which is often unavailable in rural Kenyan clinics. This is where the clinical gap widens; while the medicine exists, the infrastructure to keep it viable does not.
Similarly, maternal and neonatal sepsis—a systemic inflammatory response to infection—remains a leading killer. In the absence of sterile environments and prophylactic antibiotics, common bacteria enter the bloodstream or the newborn’s respiratory tract. This leads to septic shock, where the body’s immune response causes organ failure. The prevention is simple: clean delivery kits and timely antibiotic intervention, yet these are frequently absent in marginalized regions.
The Neonatal Crisis: Asphyxia and the “Golden Minute”
For the 92 newborns dying daily, neonatal asphyxia is a primary culprit. Asphyxia occurs when a baby does not receive enough oxygen before, during, or immediately after birth, leading to hypoxic-ischemic encephalopathy (HIE)—a condition where the brain is damaged due to lack of oxygen.
The clinical intervention required is “neonatal resuscitation,” often referred to as the Golden Minute. If a provider can clear the airway and provide positive-pressure ventilation within the first 60 seconds of life, the probability of survival increases exponentially. The tragedy in Kenya is that many births occur without a provider trained in these basic resuscitation maneuvers, turning a manageable complication into a fatal event.
“The disparity in maternal and neonatal survival is not a failure of medicine, but a failure of distribution. We have the clinical tools to stop these deaths; we lack the political and logistical will to place them in the hands of every midwife in East Africa.” — Dr. Sarah Njau, Senior Epidemiologist specializing in Maternal Health.
Global Benchmarks and the Equity Gap
When comparing Kenya’s data to global standards, the disparity is jarring. In systems like the UK’s National Health Service (NHS) or the US healthcare system, the Maternal Mortality Ratio (MMR) is a fraction of Kenya’s. This is not because Western doctors possess “miracle” drugs, but because they have integrated prenatal screening for pre-eclampsia—a condition characterized by high blood pressure and protein in the urine—which can be managed with magnesium sulfate to prevent seizures (eclampsia).
The funding for these interventions in Kenya often comes from international bodies such as the World Health Organization (WHO) and USAID. However, bias in funding often prioritizes “vertical” programs (targeting one specific disease like HIV/AIDS) over “horizontal” programs (strengthening the overall healthcare system). This leaves the general obstetric infrastructure underfunded and understaffed.
| Preventable Cause | Clinical Mechanism | Gold-Standard Intervention | Infrastructure Requirement |
|---|---|---|---|
| Postpartum Hemorrhage | Uterine Atony (Lack of contraction) | Oxytocin / Misoprostol | Cold Chain Storage |
| Eclampsia | Hypertensive Crisis / Cerebral Edema | Magnesium Sulfate | BP Monitoring / Skilled Nursing |
| Neonatal Asphyxia | Hypoxia (Oxygen deprivation) | Positive-Pressure Ventilation | Resuscitation Training |
| Sepsis | Systemic Bacterial Infection | Broad-Spectrum Antibiotics | Sterile Delivery Kits |
Contraindications & When to Consult a Doctor
While this article focuses on systemic crises, individuals experiencing pregnancy or postpartum recovery must be vigilant. Make sure to seek immediate emergency medical intervention if you experience any of the following “red flag” symptoms:
- Severe Hypertension: A sudden, blinding headache or blurred vision (potential signs of pre-eclampsia).
- Excessive Bleeding: Soaking through more than one sanitary pad per hour postpartum.
- High Fever: A temperature above 38°C (100.4°F) following delivery, which may indicate sepsis.
- Neonatal Respiratory Distress: If a newborn exhibits “grunting,” nasal flaring, or a bluish tint to the skin (cyanosis), immediate resuscitation is required.
Contraindication Note: Never administer uterotonic medications or antihypertensives without a clinical diagnosis, as incorrect dosages can lead to uterine rupture or severe hypotension.
The Path Toward Zero Preventable Deaths
Solving Kenya’s silent crisis requires more than just medicine; it requires a shift toward “Community-Based Maternal Care.” By training community health volunteers to recognize the early signs of hemorrhage and sepsis, the “First Delay” can be eliminated. Investing in solar-powered refrigeration for oxytocin would close the gap in PPH management.
The goal is not merely to increase the number of births in facilities, but to ensure those facilities are equipped to handle emergencies. When clinical competence meets accessible infrastructure, the death rate for mothers and newborns doesn’t just drop—it vanishes.
References
- World Health Organization (WHO) – Maternal Mortality Fact Sheets
- The Lancet – Global Health: Maternal and Neonatal Health Series
- PubMed – Clinical Interventions for Postpartum Hemorrhage in Low-Resource Settings
- Centers for Disease Control and Prevention (CDC) – Global Health Maternal Health Indicators