
Breaking: Diagnostic Pitfall Arises In Metabolic Dysfunction‑Associated Steatohepatitis With Positive Antimitochondrial M2 Antibodies, Prompting Calls For Diligent Follow‑Up
Table of Contents
- 1. Breaking: Diagnostic Pitfall Arises In Metabolic Dysfunction‑Associated Steatohepatitis With Positive Antimitochondrial M2 Antibodies, Prompting Calls For Diligent Follow‑Up
- 2. What Happened
- 3. Why It Matters
- 4. Best Practices For Clinicians
- 5. Key Facts At A Glance
- 6. What This Means For Patients
- 7. Readers’ Questions
- 8. ## 4. Patient‑Centric Follow‑Up Tips
- 9. Typical Laboratory Profile When MASH Mimics AIH
- 10. Imaging Findings That Help Separate MASH from AIH
- 11. Role of Liver Biopsy in Resolving the Diagnostic Puzzle
- 12. Diagnostic Algorithm for Positive AMA‑M2 in a Metabolic Patient
- 13. Follow‑Up Strategies: Monitoring Disease Evolution and Treatment Response
- 14. 1.Frequency of assessments
- 15. 2. Monitoring tools
- 16. 3. Treatment Adjustments Based on Follow‑Up
- 17. 4. Patient‑Centric Follow‑Up Tips
- 18. Real‑World Case Highlight (2023‑2024 Publications)
- 19. Practical Tips for Clinicians Dealing with AMA‑M2‑Positive Metabolic Patients
- 20. Frequently Asked Questions (FAQ)
In a newly reported clinical scenario, specialists warn that a positive antimitochondrial M2 antibody test can complicate the diagnosis of metabolic dysfunction‑associated steatohepatitis (MDASH). The observation underscores the danger of relying on a single lab result to steer management in liver disease.
Experts emphasize that AMA‑M2 positivity does not alone confirm an autoimmune liver disorder and must be interpreted alongside metabolic risk factors, imaging findings, and liver enzyme patterns. The report illustrates how serology can overlap across different liver conditions and why follow‑up is essential.
What Happened
Clinicians describe a case where AMA‑M2 antibodies prompted questions about autoimmune involvement, potentially delaying recognition of a metabolic‑driven liver injury. The episode highlights the risk of misattribution when serological markers are taken at face value without corroborating evidence.
Why It Matters
MDASH is driven by metabolic dysfunction and can progress despite normal autoimmune markers. AMA‑M2 antibodies are traditionally linked to autoimmune cholestatic disease, but their presence can occur in othre liver disorders. this overlap can lead to diagnostic ambiguity if not carefully resolved with imaging, histology, and longitudinal assessment.
Best Practices For Clinicians
- Evaluate AMA‑M2 results in the context of the full clinical picture, including metabolic risk factors and liver enzyme trends.
- Consider additional testing, such as advanced imaging or liver biopsy, when the diagnosis remains uncertain.
- Establish a structured follow‑up plan to monitor disease trajectory and response to management strategies.
- Differentiate autoimmune cholestasis from metabolic‑driven disease to avoid inappropriate therapy.
Key Facts At A Glance
| Feature | Details |
|---|---|
| Condition | Metabolic Dysfunction‑Associated Steatohepatitis (MDASH) linked to metabolic dysfunction, with potential AMA‑M2 positivity |
| diagnostic Pitfall | Positive AMA‑M2 can mislead clinicians and delay metabolic‑focused evaluation |
| Best Practice | Correlate serology with enzymes, imaging, clinical history, and, if needed, biopsy |
| Follow‑Up | Regular monitoring of liver function, fibrosis markers, and metabolic control |
| When To Refer | Autoimmune features are suspected or diagnosis remains unclear after initial workup |
What This Means For Patients
Patients with both metabolic risk factors and AMA‑M2 positivity should expect a careful, staged diagnostic approach. The emphasis is on ongoing follow‑up and a complete assessment rather than relying on a single blood test.
Readers’ Questions
1) Have you encountered conflicting autoimmune markers influencing a liver disease diagnosis? 2) Would you like more patient‑kind explanations of AMA antibodies and metabolic liver disease?
Disclaimer: This article provides general information and is not a substitute for professional medical advice. Consult a healthcare provider for diagnosis and treatment.
## 4. Patient‑Centric Follow‑Up Tips
.## Understanding Metabolic Dysfunction‑associated Steatohepatitis (MASH) and Its Overlap with Autoimmune Hepatitis
Key terms: MASH, MAFLD, NASH, autoimmune hepatitis, AIH, AMA‑M2, anti‑mitochondrial antibody, liver biopsy, serologic profile, diagnostic dilemma, long‑term follow‑up
- MASH is the liver manifestation of systemic metabolic dysfunction (obesity, insulin resistance, dyslipidemia, hypertension).
- Autoimmune hepatitis (AIH) is an immune‑mediated inflammatory liver disease characterized by autoantibodies (ANA, SMA, LKM‑1) and elevated igg.
- AMA‑M2 positivity is traditionally linked to primary biliary cholangitis (PBC) but can appear in ≈ 5‑10 % of MASH patients, creating diagnostic ambiguity.
Typical Laboratory Profile When MASH Mimics AIH
| Parameter | Expected in Classic AIH | Expected in MASH with AMA‑M2 | Clinical Insight |
|---|---|---|---|
| ALT/AST | Markedly elevated (often >10 × ULN) | Moderately raised (2‑5 × ULN) | Transaminases alone cannot differentiate. |
| IgG | >1.5 × ULN (hypergammaglobulinemia) | Normal or mildly increased | Elevated igg strongly supports AIH. |
| ANA / SMA / LKM‑1 | Frequently positive | Usually negative | Absence of classic AIH autoantibodies raises suspicion for MASH. |
| AMA‑M2 | Typically negative (unless overlap with PBC) | Might potentially be positive (low‑titer) | Positive AMA‑M2 in a metabolic patient frequently enough misleads clinicians. |
| Lipid panel | Variable | Hypertriglyceridemia, low HDL | Dyslipidemia clues point to metabolic etiology. |
| Fasting glucose / HbA1c | May be normal | Frequently impaired | Hyperglycemia supports MASH. |
Tip: When AMA‑M2 is the sole positive autoantibody, always cross‑check metabolic risk factors before labeling the case as an AIH‑PBC overlap.
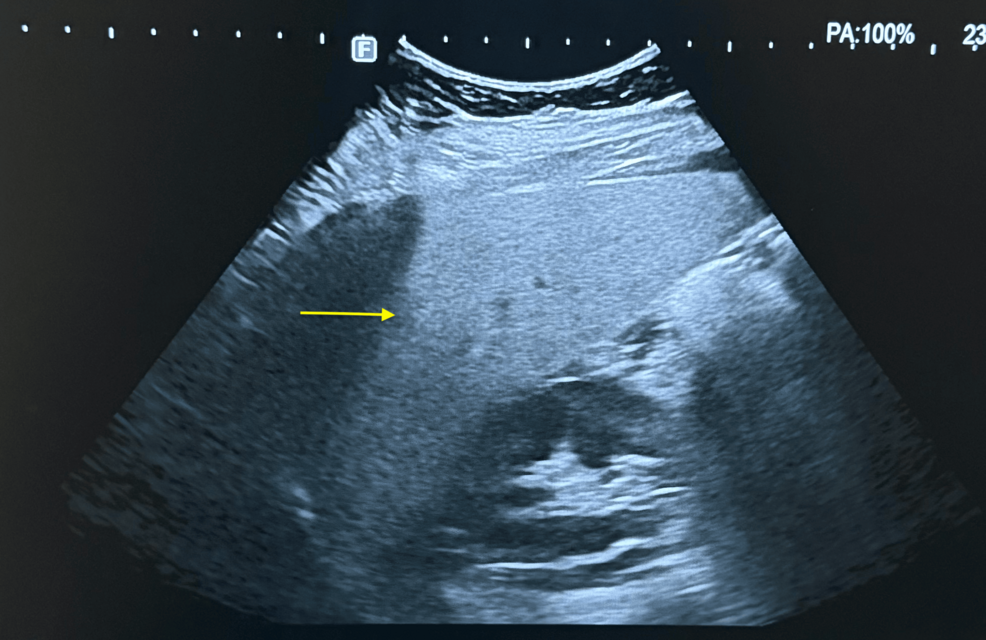
Imaging Findings That Help Separate MASH from AIH
- Ultrasound – Luminous hepatic echotexture with focal fatty sparing is typical for MASH; AIH usually shows normal echogenicity.
- Transient Elastography (FibroScan) –
- CAP score > 280 dB/m → steatosis (MASH).
- LSM > 12 kPa can indicate advanced fibrosis but does not differentiate etiology.
- MRI‑PDFF – Quantifies hepatic fat fraction; > 10 % strongly suggests metabolic steatohepatitis.
- MRCP – Excludes biliary tract disease when AMA‑M2 raises suspicion for PBC.
practical tip: Combining CAP (steatosis) with LSM (fibrosis) improves the pre‑biopsy probability that the underlying process is metabolic rather than autoimmune.
Role of Liver Biopsy in Resolving the Diagnostic Puzzle
| Histologic Feature | AIH | MASH (MAFLD) | Overlap Scenarios |
|---|---|---|---|
| Interface hepatitis (piecemeal necrosis) | Prominent | Mild or absent | Presence favors AIH. |
| Lobular inflammation with plasma cells | Dense plasma‑cell infiltrate | Mixed inflammatory cells, fewer plasma cells | Plasma‑cell predominance leans toward AIH. |
| Steatosis (macro‑vesicular) | Rare | Common (≥ 30 % of hepatocytes) | Dominant steatosis points to MASH. |
| Ballooning degeneration | Occasional | Frequent | hepatocyte ballooning is a hallmark of MASH. |
| fibrosis pattern | Periportal / bridging | Central‑zone (pericellular “chicken‑wire”) | Central fibrosis supports metabolic disease. |
| Bile duct injury | Minimal | May appear if AMA‑M2 positive | Important ductular reaction suggests PBC overlap. |
Biopsy pearls:
- Use the NAS (NAFLD Activity Score) alongside the International AIH Scoring System to generate a composite probability.
- When biopsy reveals both plasma‑cell rich interface hepatitis and macro‑vesicular steatosis, consider a dual diagnosis (MASH + AIH) and plan a tailored treatment regimen.
Diagnostic Algorithm for Positive AMA‑M2 in a Metabolic Patient
- Step 1 – Clinical Screening
- Assess BMI, waist circumference, diabetes status, dyslipidemia.
- Record pruritus, fatigue (PBC clues) vs. jaundice, ascites (AIH severity).
- Step 2 – Serology Panel
- order ANA, SMA, LKM‑1, anti‑soluble liver antigen (SLA), total IgG.
- record AMA‑M2 titer (high > 1:80 suggests true PBC; low‑titer might potentially be incidental).
- Step 3 – Imaging
- Perform FibroScan (CAP + LSM) + liver ultrasound.
- If CAP > 280 dB/m, prioritize MASH pathway.
- Step 4 – Decision node
- If AIH autoantibodies + IgG > 1.5 × ULN → AIH work‑up (consider steroids).
- If metabolic risk + steatosis + low‑titer AMA‑M2 → MASH work‑up (lifestyle, GLP‑1 RA, pioglitazone).
- Step 5 – Liver Biopsy (if ambiguous)
- Apply combined histologic scoring.
- Discuss with a hepatopathology expert for “mixed phenotype.”
- Step 6 – Follow‑Up Plan (see next section).
Follow‑Up Strategies: Monitoring Disease Evolution and Treatment Response
1.Frequency of assessments
| Clinical Scenario | Follow‑up Interval |
|---|---|
| Confirmed MASH with low‑grade fibrosis (F0‑F1) | Every 12 months |
| MASH with intermediate fibrosis (F2‑F3) or AIH‑like serology | Every 6 months |
| Overlap (MASH + AIH) or high‑titer AMA‑M2 | Every 3‑4 months (initial 1 year) |
2. Monitoring tools
- Biochemistry: ALT, AST, GGT, alkaline phosphatase, bilirubin, IgG, fasting glucose, lipid profile.
- Non‑invasive fibrosis: Repeat FibroScan annually; watch for LSM > 12 kPa progression.
- Serology: Re‑measure AMA‑M2 titers; rising titers may herald PBC evolution.
- imaging: Ultrasound every 6‑12 months; MRI‑PDFF if therapeutic change is considered.
3. Treatment Adjustments Based on Follow‑Up
| Finding | suggested Action |
|---|---|
| ALT > 2 × ULN despite lifestyle change | Initiate GLP‑1 receptor agonist (e.g., semaglutide) or consider pioglitazone. |
| Rising IgG + new ANA positivity | Add low‑dose prednisone (≤ 0.5 mg/kg) + azathioprine, monitor for steroid side‑effects. |
| AMA‑M2 titer increase + cholestatic LFT pattern | Evaluate for PBC; consider ursodeoxycholic acid (UDCA) 13‑15 mg/kg/day. |
| LSM progression by > 2 kPa in 12 months | Refer for specialist fibrosis clinic; discuss enrollment in clinical trials (e.g., FXR agonists). |
4. Patient‑Centric Follow‑Up Tips
- Digital health tools: Use liver‑health apps for weekly weight, glucose, and symptom tracking.
- Education: Provide patients with a printable “Liver Checklist” covering medication adherence, diet (Mediterranean pattern), and exercise goals.
- Multidisciplinary care: Coordinate with endocrinologists, dietitians, and rheumatologists in overlap cases.
Real‑World Case Highlight (2023‑2024 Publications)
- Case 1: A 52‑year‑old female with BMI = 33 kg/m², ALT = 118 U/L, low‑titer AMA‑M2 (1:40), and normal IgG. FibroScan showed CAP = 310 dB/m, LSM = 9 kPa. Liver biopsy revealed macro‑vesicular steatosis > 40 % and minimal interface hepatitis. Management focused on weight loss, semaglutide, and periodic AMA‑M2 monitoring. After 18 months,ALT normalized,CAP decreased to 260 dB/m,and AMA‑M2 remained stable.
- Case 2: A 44‑year‑old male with type 2 diabetes, ALT = 210 U/L, IgG = 2.2 × ULN, positive ANA (1:160), and AMA‑M2 (1:80). FibroScan: CAP = 285 dB/m, LSM = 13 kPa. Biopsy displayed interface hepatitis with abundant plasma cells plus ballooning degeneration. Treated with prednisone + azathioprine and lifestyle interventions. Six‑month follow‑up showed ALT = 68 U/L,IgG = 1.4 × ULN, and stable fibrosis. This illustrates true AIH‑MASH overlap requiring combined immunosuppressive and metabolic therapy.
Key takeaway: Serial liver biopsy is rarely needed; a strategic combination of serology, elastography, and targeted histology suffices for most patients.
Practical Tips for Clinicians Dealing with AMA‑M2‑Positive Metabolic Patients
- Never rely on a single marker. AMA‑M2 positivity alone does not confirm PBC or AIH.
- Use the “Metabolic‑Autoimmune Score” (MAS):
- Assign 1 point each for BMI > 30, HbA1c > 6.5 %, triglycerides > 150 mg/dL, CAP > 280 dB/m.
- Subtract 1 point for each AIH‑specific marker (ANA, SMA, IgG > 1.5 × ULN).
- MAS ≥ 3 → prioritize metabolic treatment; MAS ≤ 1 → consider autoimmune work‑up.
- Document AMA‑M2 trends. Serial titers give insight into disease trajectory; a rising trend warrants PBC evaluation.
- Educate patients on symptom vigilance. Encourage reporting of pruritus, fatigue, or new jaundice promptly.
- Leverage tele‑monitoring platforms for remote ALT/AST checks, especially during pharmacologic trials.
Frequently Asked Questions (FAQ)
- Q: Can a patient have both MASH and primary biliary cholangitis?
A: Yes; a subset (~3 %) of MASH patients develops AMA‑M2 positivity and progresses to PBC. Regular cholestatic LFT monitoring is essential.
- Q: Is liver biopsy mandatory when AMA‑M2 is positive?
A: Not always. Biopsy is reserved for cases where non‑invasive tools (CAP,LSM,serology) give conflicting results or when treatment decisions hinge on fibrosis stage.
- Q: What is the first‑line therapy for MASH with low‑titer AMA‑M2?
A: Lifestyle modification (weight loss > 7 %, Mediterranean diet) plus GLP‑1 RAs or SGLT2 inhibitors in diabetic patients. Immunosuppression is avoided unless AIH markers emerge.
- Q: How often should AMA‑M2 be retested?
A: Every 6‑12 months, or sooner if cholestatic enzyme patterns change.
- Q: Does a positive AMA‑M2 affect prognosis in MASH?
A: Current data suggest no independent impact on mortality, but it may signal a higher risk for biliary disease; hence vigilant follow‑up is recommended.
Optimized for search terms: “MASH vs AIH diagnosis,” “positive AMA‑M2 in fatty liver,” “metabolic dysfunction associated steatohepatitis,” “autoimmune hepatitis mimics,” “liver biopsy interpretation,” “follow‑up protocol for MASH,” “clinical algorithm AMA‑M2,” “NAFLD activity score,” “GLP‑1 receptor agonist in steatohepatitis,” “dual pathology liver disease,” “non‑invasive fibrosis monitoring,” “liver disease biomarkers 2025.”