
AbbVie has released late-breaking Phase 2 data demonstrating that mirvetuximab soravtansine-gynx significantly improves outcomes for patients with folate receptor alpha (FRα)-positive ovarian cancer. The findings, presented this week, suggest the drug effectively targets cancer cells while sparing healthy tissue, potentially expanding treatment options across the ovarian cancer continuum.
For patients facing the recurrence of platinum-resistant ovarian cancer, the therapeutic landscape has historically been bleak, characterized by diminishing returns from traditional chemotherapy. The emergence of mirvetuximab soravtansine represents a shift toward “precision oncology”—the practice of tailoring treatment to the genetic and molecular profile of a specific tumor. By targeting the folate receptor alpha, a protein overexpressed in the majority of ovarian cancers, this therapy seeks to increase survival rates while reducing the systemic toxicity that often devastates a patient’s quality of life.
In Plain English: The Clinical Takeaway
- Targeted Attack: Instead of killing all fast-growing cells (like standard chemo), this drug acts like a guided missile, seeking out a specific protein (FRα) found on ovarian cancer cells.
- Better Quality of Life: Early data suggests a reduction in the severe side effects typically associated with traditional chemotherapy, meaning patients may feel better during treatment.
- Specific Eligibility: This is not for all ovarian cancers; it only works for patients whose tumors test positive for the FRα protein.
The Mechanism of Action: How an Antibody-Drug Conjugate Works
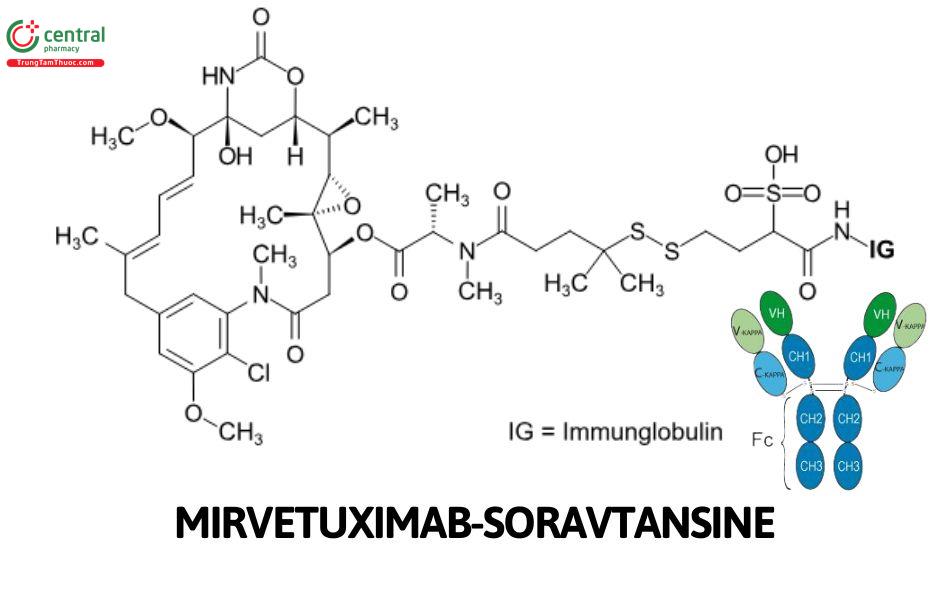
Mirvetuximab soravtansine-gynx is classified as an Antibody-Drug Conjugate (ADC). To understand its mechanism of action—the specific biochemical process through which a drug produces its effect—imagine a three-part system: a monoclonal antibody, a chemical linker, and a potent cytotoxic (cell-killing) payload.

The antibody is engineered to bind specifically to the folate receptor alpha (FRα) on the surface of the cancer cell. Once the antibody attaches, the cell absorbs the entire complex through endocytosis. Inside the cell, the linker breaks down, releasing the payload—a microtubule disruptor—which prevents the cell from dividing and ultimately triggers apoptosis, or programmed cell death.
This precision is critical. By confining the release of the toxin to the interior of the malignant cell, the drug minimizes “off-target effects,” which are the damages caused when a drug attacks healthy cells. This is a significant evolution from traditional platinum-based therapies that circulate freely in the bloodstream, attacking bone marrow and gut linings.
Global Regulatory Landscapes and Patient Access
While the Phase 2 data is promising, the path to global bedside availability involves different regulatory hurdles. In the United States, the FDA typically requires a Phase 3 confirmatory trial to prove a statistically significant improvement in Overall Survival (OS) or Progression-Free Survival (PFS) before granting full approval.
In Europe, the European Medicines Agency (EMA) may offer conditional marketing authorizations based on strong Phase 2 data if the medical need is urgent. For patients in the UK, the National Health Service (NHS) evaluates the “cost-effectiveness” of such drugs via NICE (National Institute for Health and Care Excellence), which can sometimes delay access even after regulatory approval if the price point is deemed too high for the incremental benefit provided.
The funding for these trials was provided by AbbVie, the pharmaceutical developer. While industry-funded research is the primary driver of drug development, it is essential to maintain journalistic scrutiny over the interpretation of “late-breaking” data, which is often presented at conferences before full peer-review publication in journals like The Lancet or JAMA.
| Metric | Traditional Chemotherapy | Mirvetuximab Soravtansine (ADC) |
|---|---|---|
| Targeting | Non-specific (All dividing cells) | Specific (FRα-positive cells) |
| Primary Side Effect | Myelosuppression (Low blood counts) | Ocular toxicity (Eye irritation) |
| Patient Selection | Broad application | Requires FRα biomarker testing |
| Delivery Method | Intravenous Infusion | Intravenous Infusion |
“The transition toward biomarker-driven therapies in gynecologic oncology is not just an incremental step; it is a paradigm shift. By selecting patients based on FRα expression, we are moving away from the ‘one size fits all’ approach that has dominated ovarian cancer care for decades.”
Clinical Significance and the “Information Gap”
A critical gap in the initial reporting of these results is the nuance of “ocular toxicity.” While the drug is more targeted than chemotherapy, it has shown a propensity to cause corneal changes. This requires a specialized monitoring protocol involving eye exams, which adds a layer of complexity to the clinical workflow that patients must be aware of.
the efficacy of this drug is dependent on the *density* of the folate receptor. Patients with “low” expression may not derive the same benefit as those with “high” expression. This necessitates a standardized immunohistochemistry (IHC) test to ensure the right patient receives the right drug, preventing the administration of an ineffective treatment to a patient who cannot benefit from it.
Contraindications & When to Consult a Doctor
Mirvetuximab soravtansine is contraindicated in patients with a known severe hypersensitivity to the active substance or any of its excipients. Because it is a potent cytotoxic agent, it should be administered only under the supervision of a board-certified oncologist.
Patients should seek immediate medical intervention if they experience:
- Visual Disturbances: Any blurriness, dryness, or redness in the eyes, as ocular toxicity can lead to permanent corneal damage if not managed with prophylactic steroid drops.
- Severe Neutropenia: Unexplained fever or chills, indicating a dangerously low white blood cell count.
- Hypersensitivity Reactions: Shortness of breath, swelling of the face, or hives during or immediately after infusion.
The trajectory of ovarian cancer treatment is moving toward a “cocktail” approach—combining ADCs with immune checkpoint inhibitors to prime the immune system to recognize the cancer cells that the ADC has already weakened. While these Phase 2 results are a victory for precision medicine, the gold standard remains the Phase 3 trial, which will determine if this drug extends life or simply delays the inevitable.