

Iptacopan, a novel oral inhibitor of the alternative complement pathway, has demonstrated sustained kidney function benefits and a reduction in proteinuria in patients with IgA nephropathy (IgAN) over a 24-month period, as detailed in recently published data. This represents a potential new treatment option for a disease affecting millions globally, offering hope for slowing disease progression and delaying the need for dialysis. The findings were presented this week in the New England Journal of Medicine.
IgA nephropathy is a chronic autoimmune disease where deposits of immunoglobulin A (IgA), an antibody, build up in the kidneys, leading to inflammation and gradual loss of kidney function. Currently, treatment focuses on managing symptoms like high blood pressure and proteinuria (protein in the urine) with medications like ACE inhibitors and corticosteroids. However, these treatments don’t address the underlying cause of the disease and can have significant side effects. Iptacopan targets the alternative complement pathway, a part of the immune system that plays a key role in the inflammation driving IgAN. By blocking this pathway, iptacopan aims to reduce kidney damage.
In Plain English: The Clinical Takeaway
- What it is: Iptacopan is a pill that helps protect your kidneys in a specific autoimmune kidney disease called IgA nephropathy.
- How it works: It calms down an overactive part of your immune system that’s attacking your kidneys.
- What the study showed: People taking iptacopan had slower kidney damage and less protein in their urine compared to those on standard treatment.
Understanding the Mechanism: Complement Inhibition and IgAN
The alternative complement pathway is a crucial component of the innate immune system, providing rapid defense against pathogens. However, in IgAN, it becomes dysregulated, contributing to inflammation and glomerular damage. Iptacopan specifically inhibits factor B, a key protein in this pathway, effectively “switching off” the damaging cascade. This differs from other complement inhibitors, which target C5, a later stage in the pathway. Targeting factor B offers a more proximal block, potentially leading to greater efficacy and a different side effect profile. The Phase III clinical trial, known as ACCEPT-IgAN, enrolled 336 patients with biopsy-proven IgAN and persistent proteinuria despite standard treatment. Participants were randomized to receive either iptacopan 200mg twice daily or placebo, in addition to standard care.
24-Month Data: Efficacy and Safety Profile
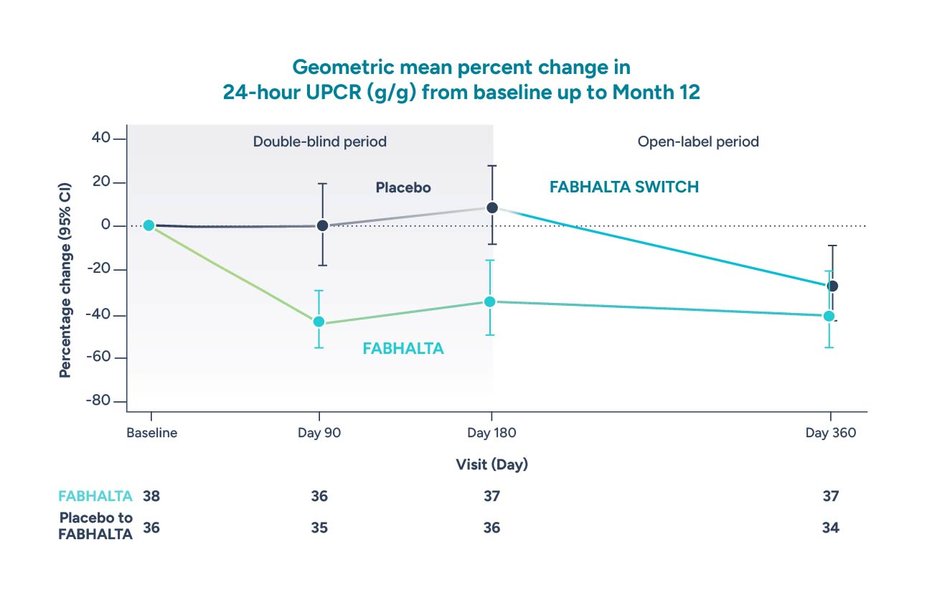
The 24-month data, published this week, builds upon the promising initial results from the ACCEPT-IgAN trial. Researchers observed a statistically significant and clinically meaningful reduction in proteinuria in the iptacopan group compared to placebo (mean reduction of 45.2% vs. 14.4%, p<0.001). Importantly, the treatment group also demonstrated a slower rate of estimated glomerular filtration rate (eGFR) decline – a measure of kidney function – compared to the placebo group. While the initial data showed a higher rate of serious infections in the iptacopan group, the 24-month data suggests this risk may be manageable with appropriate monitoring and preventative measures.
| Endpoint | Iptacopan (N=168) | Placebo (N=168) | p-value |
|---|---|---|---|
| Change in Proteinuria (mg/g creatinine) | -45.2% | -14.4% | <0.001 |
| eGFR Slope (mL/min/1.73m2/year) | -2.88 | -5.47 | 0.001 |
| Serious Infections (%) | 8.3% | 4.8% | 0.21 |
Global Impact and Regulatory Pathways
IgAN affects an estimated 1.6 million people in the United States and is particularly prevalent in certain populations, including individuals of Asian and Hispanic descent. The National Kidney Foundation estimates that IgAN is responsible for approximately 10% of all cases of conclude-stage renal disease (ESRD). In Europe, prevalence rates vary, but IgAN remains a significant cause of glomerulonephritis. The European Medicines Agency (EMA) is currently reviewing the data submitted by Novartis, the manufacturer of iptacopan, with a decision expected in the coming months. In the United States, Novartis submitted a New Drug Application (NDA) to the Food and Drug Administration (FDA) in late 2025 and a decision is anticipated in the first half of 2027. Approval would significantly alter the treatment landscape for IgAN, offering a targeted therapy to slow disease progression. Access to iptacopan will likely be tiered based on national healthcare systems; the NHS in the UK, for example, will conduct a cost-effectiveness analysis before making a decision on reimbursement.
The research was funded by Novartis, which also sponsored the ACCEPT-IgAN trial. This funding source is publicly disclosed in the New England Journal of Medicine publication. It’s crucial to acknowledge this potential for bias, although the rigorous design of the trial – including its double-blind, placebo-controlled nature – mitigates some of these concerns.
“The 24-month data reinforces the potential of iptacopan to address a significant unmet need in IgA nephropathy,” says Dr. Maria Rodriguez-Porcel, a leading nephrologist at the University of Barcelona, who was not involved in the study. “The sustained reduction in proteinuria and slower decline in kidney function are clinically meaningful outcomes that could translate to improved long-term patient outcomes.”
Contraindications & When to Consult a Doctor
Iptacopan is not suitable for everyone. Individuals with a history of severe infections, particularly those caused by encapsulated bacteria (like pneumococcus), should avoid this medication due to the increased risk of infection associated with complement inhibition. Patients with active tuberculosis or other serious infections should also not receive iptacopan. It is essential to inform your doctor about all existing medical conditions and medications before starting iptacopan. Consult a doctor immediately if you experience symptoms of infection, such as fever, chills, cough, or sore throat, while taking iptacopan. Regular monitoring of blood counts and liver function is also recommended.
Looking ahead, further research is needed to determine the optimal duration of iptacopan treatment and to identify biomarkers that can predict which patients are most likely to benefit. Long-term studies are also crucial to assess the long-term safety and efficacy of iptacopan and to evaluate its impact on cardiovascular outcomes, which are a major concern in patients with chronic kidney disease. The advent of iptacopan marks a significant step forward in the treatment of IgAN, offering a new avenue for preserving kidney function and improving the lives of those affected by this debilitating disease.