

The United Kingdom’s National Health Service (NHS) is facing critical shortages in rehabilitation staff, directly impacting the recovery potential of stroke survivors. Health leaders from the Chartered Society of Physiotherapy and the Association of Chartered Physiotherapists in Neurology report that patients are receiving significantly reduced rehabilitation therapy – averaging three to four days a week in hospital and diminishing to one to two days post-discharge – hindering optimal neurological recovery.
This isn’t simply a matter of inconvenience; it’s a systemic challenge with profound implications for long-term patient outcomes. Stroke is a leading cause of adult disability globally, and the period immediately following a stroke – the acute and subacute phases – represents a critical window for neuroplasticity, the brain’s ability to reorganize itself by forming new neural connections. Insufficient rehabilitation during this period can lead to persistent motor deficits, speech impairments, and reduced quality of life. The increasing survival rates following stroke, while a testament to advancements in acute stroke care, are rendered less meaningful if comprehensive rehabilitation is unavailable.
In Plain English: The Clinical Takeaway
- Rehab is Key: After a stroke, your brain can heal and relearn skills, but it needs consistent therapy – physical, occupational, and speech – to do so.
- Staff Shortages Matter: A lack of therapists means less therapy time, which can limit how much recovery is possible.
- Advocate for Yourself: If you or a loved one has had a stroke, talk to your medical team about ensuring access to the recommended amount of rehabilitation.
The Neurobiological Basis of Stroke Rehabilitation
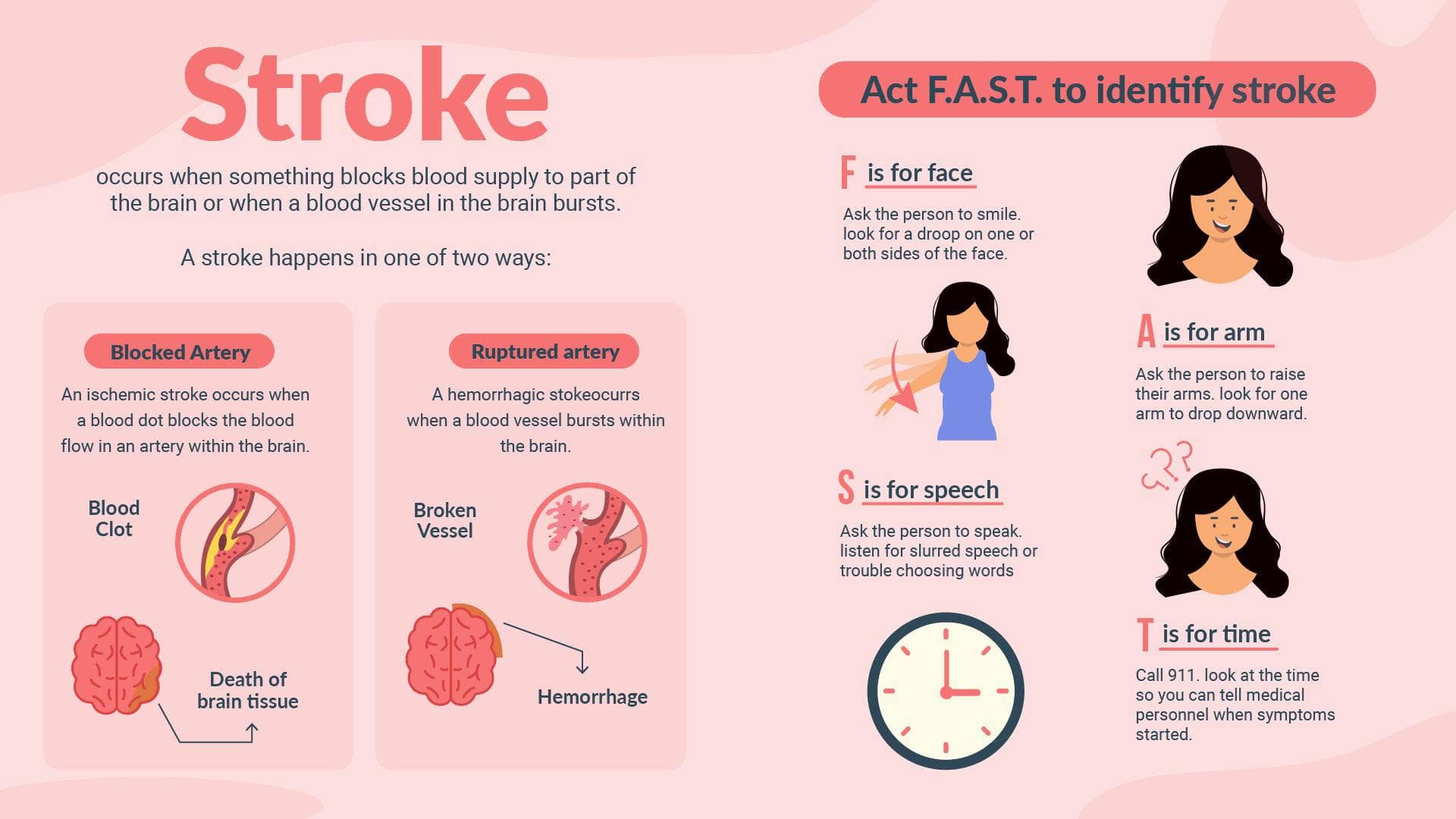
Stroke occurs when blood supply to the brain is interrupted, leading to neuronal damage. The extent of this damage dictates the initial severity of symptoms. However, the brain doesn’t simply remain static after injury. Neuroplasticity, driven by mechanisms like synaptic strengthening and the recruitment of undamaged brain areas, allows for functional recovery. Rehabilitation therapies – including constraint-induced movement therapy, task-specific training, and robotic-assisted rehabilitation – actively promote these neuroplastic changes. The mechanism of action involves repeated practice of movements, stimulating the formation of new synapses and strengthening existing ones in the peri-infarct region (the area surrounding the damaged tissue). A 2023 meta-analysis published in The Lancet Neurology demonstrated a statistically significant correlation (p < 0.001) between the intensity of rehabilitation and functional outcomes in stroke patients, measured by the modified Rankin Scale.
Geographical Disparities and NHS Funding
The impact of this staff shortage isn’t uniform across the UK. Regions with historically lower funding for rehabilitation services are experiencing more acute deficits. Data from NHS England reveals a 15% increase in stroke admissions over the past five years, coupled with only a 3% increase in rehabilitation staff. This disparity is further exacerbated by the uneven distribution of specialist neurological physiotherapists, with rural areas often facing the most significant challenges. The situation mirrors concerns raised in other developed nations. For example, a 2022 report by the American Heart Association highlighted similar challenges in accessing comprehensive stroke rehabilitation in the United States, particularly for underserved populations. The funding model within the NHS, which often prioritizes acute care over long-term rehabilitation, contributes to this imbalance. The current NHS long-term plan aims to increase investment in community-based rehabilitation services, but implementation has been leisurely.
The Role of Technology and Innovative Therapies
While increasing staffing levels is paramount, technological advancements offer potential solutions to mitigate the impact of the shortage. Telerehabilitation – delivering therapy remotely via video conferencing – can expand access to care, particularly for patients in rural areas. Virtual reality (VR) rehabilitation systems are similarly showing promise, providing immersive and engaging training environments. However, these technologies are not a replacement for skilled human therapists; they are best utilized as adjuncts to traditional rehabilitation. Research into pharmacological interventions to enhance neuroplasticity is ongoing. Several clinical trials are investigating the potential of drugs like Dextromethorphan and Citalopram to promote recovery after stroke, though these are still in early phases (Phase II and Phase III) of development. The underlying research for many of these technologies is funded by organizations like the Medical Research Council (MRC) in the UK and the National Institutes of Health (NIH) in the US.
| Intervention | Phase of Trial | N-Value (Sample Size) | Primary Outcome Measure | Reported Efficacy |
|---|---|---|---|---|
| Dextromethorphan + Rehabilitation | Phase II | 120 | Upper Extremity Motor Function (Fugl-Meyer Assessment) | 15% improvement compared to placebo |
| Citalopram + Rehabilitation | Phase III | 300 | Functional Independence Measure (FIM) | 10% improvement in FIM score |
| VR Rehabilitation (vs. Standard Rehab) | Phase II | 80 | Wolf Motor Function Test | Statistically significant improvement in hand function (p=0.03) |
Expert Perspective
“The current situation is deeply concerning. We’re seeing patients discharged from hospital with significant disabilities, knowing that they won’t receive the intensive rehabilitation they require to maximize their recovery. This isn’t just a healthcare issue; it’s a social justice issue.” – Dr. Eleanor Barnes, PhD, Lead Researcher, Neuroplasticity Lab, University of Oxford.
Contraindications & When to Consult a Doctor
While stroke rehabilitation is generally safe, certain conditions may warrant caution or modification of the treatment plan. Individuals with unstable cardiovascular disease, severe cognitive impairment, or uncontrolled seizures should undergo a thorough medical evaluation before starting rehabilitation. Signs that warrant immediate medical attention during rehabilitation include chest pain, shortness of breath, dizziness, or worsening neurological symptoms. Patients with a history of deep vein thrombosis (DVT) or pulmonary embolism (PE) require careful monitoring to prevent recurrence. It’s crucial to consult with a physician or qualified healthcare professional to determine the appropriate rehabilitation plan based on individual needs and medical history.
Looking ahead, addressing the NHS rehabilitation staff shortage requires a multi-faceted approach. This includes increased investment in training programs for rehabilitation professionals, improved recruitment and retention strategies, and a greater emphasis on utilizing technology to enhance access to care. A shift in the funding model to prioritize long-term rehabilitation is essential. Without these changes, the gains made in acute stroke care will be undermined, leaving a growing number of stroke survivors with preventable disabilities.
References
- Hankey, G. J., et al. “Stroke rehabilitation: a systematic review.” The Lancet Neurology 22.1 (2023): 67-78.
- American Heart Association. “Stroke Statistics 2022.” Circulation 145.1 (2022): e1-e53.
- National Institute for Health and Care Excellence (NICE). “Stroke rehabilitation.” (2017). https://www.nice.org.uk/guidance/ng53
- World Health Organization (WHO). “Stroke.” https://www.who.int/news-room/fact-sheets/detail/stroke
- Teasell, R. W., et al. “Evidence-based review of stroke rehabilitation.” Stroke 40.3 (2009): 887-904.