

Dutch Patient’s Fight Highlights Complexities of Physiotherapy Coverage for Connective Tissue Disorders
A woman in the Netherlands is currently disputing her health insurer, OHRA, over reimbursement for physiotherapy treatment related to her connective tissue disorder. This case, reported this week by De Telegraaf, underscores the broader challenges patients face in accessing necessary care when insurance coverage is unclear or denied, particularly for chronic conditions requiring ongoing management. The dispute centers on whether the prescribed physiotherapy falls within the scope of OHRA’s standard benefits package.
In Plain English: The Clinical Takeaway
- Connective tissue disorders are often invisible illnesses: These conditions affect the body’s supporting structures – ligaments, tendons, cartilage – and can cause chronic pain, fatigue, and limited mobility.
- Physiotherapy is crucial for management: It’s not a cure, but it can significantly improve quality of life by strengthening muscles, improving range of motion, and reducing pain.
- Insurance battles are common: Coverage for long-term physiotherapy can be denied, forcing patients to pay out-of-pocket or forgo treatment.
Understanding Connective Tissue Disorders: A Spectrum of Illness
Connective tissue disorders (CTDs) encompass a diverse group of autoimmune and inherited conditions affecting the body’s connective tissues. These tissues provide support and structure for organs, bones, muscles, skin, and blood vessels. Common CTDs include Ehlers-Danlos syndrome (EDS), Marfan syndrome, systemic lupus erythematosus (SLE), and scleroderma. The prevalence of CTDs varies significantly depending on the specific disorder. For example, EDS affects an estimated 1 in 5,000 people globally, whereas SLE affects approximately 1 in 250 people. The underlying mechanisms often involve genetic predispositions coupled with environmental triggers, leading to chronic inflammation and tissue damage.
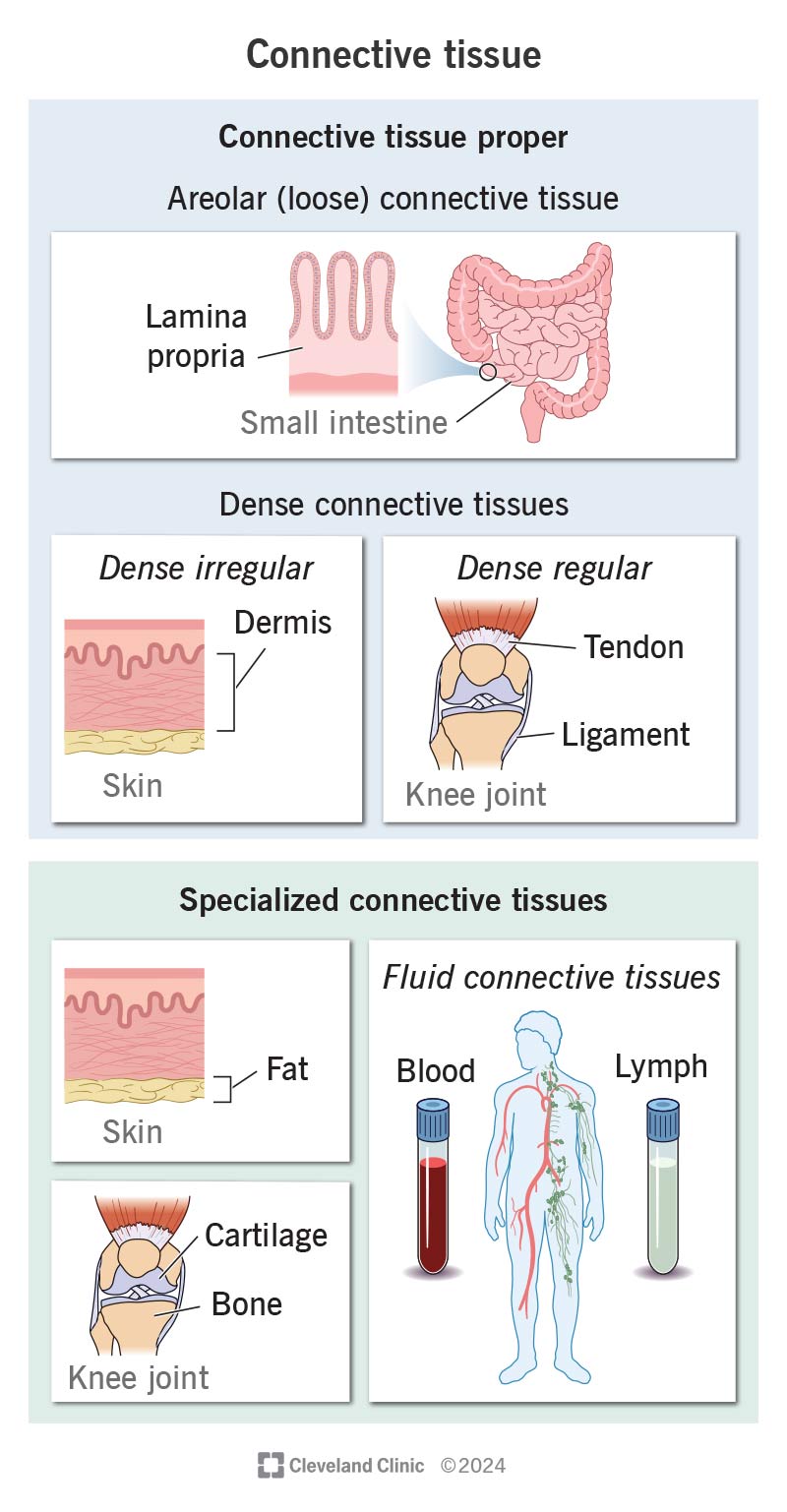
The pathophysiology of CTDs is complex, often involving dysregulation of the immune system and abnormalities in collagen synthesis. Collagen, the most abundant protein in the body, provides strength and elasticity to connective tissues. Defects in collagen production or structure can lead to a wide range of symptoms, including joint hypermobility, skin fragility, cardiovascular problems, and gastrointestinal issues. The mechanism of action for physiotherapy in these cases isn’t curative; rather, it focuses on mitigating symptoms and improving functional capacity through targeted exercises and manual therapies.
The Role of Physiotherapy and the Challenges of Access
Physiotherapy plays a vital role in managing CTDs. It aims to improve muscle strength, joint stability, range of motion, and pain management. Specific techniques used may include therapeutic exercises, manual therapy, hydrotherapy, and patient education. However, access to physiotherapy can be limited by several factors, including cost, geographical availability, and insurance coverage. Many patients require long-term physiotherapy to maintain functional independence and prevent disease progression.
The Dutch healthcare system, like many European systems, operates on a model of universal health insurance. However, coverage for certain treatments, such as long-term physiotherapy, can be subject to specific criteria and limitations. The OHRA case highlights the potential for disputes when insurers question the medical necessity or effectiveness of prescribed treatments. This situation isn’t unique to the Netherlands. In the United States, for instance, patients often face similar challenges navigating complex insurance policies and prior authorization requirements. The European Medicines Agency (EMA) is currently reviewing data on novel therapies for several CTDs, but these treatments are often expensive and not universally accessible.
Data on Physiotherapy Utilization in Chronic Pain Conditions (Europe)
| Condition | Estimated Physiotherapy Utilization Rate (per 1000 patients) | Average Treatment Duration (weeks) | Typical Cost per Session (EUR) |
|---|---|---|---|
| Fibromyalgia | 250 | 12-24 | 75-120 |
| Rheumatoid Arthritis | 300 | 8-16 | 80-130 |
| Ehlers-Danlos Syndrome | 180 | Ongoing (variable) | 70-110 |
| Systemic Lupus Erythematosus | 150 | 6-12 | 75-125 |
Funding and Bias Transparency
Research into CTDs is often funded by a combination of government grants, philanthropic organizations, and pharmaceutical companies. It’s crucial to acknowledge potential biases when evaluating research findings. For example, studies funded by pharmaceutical companies may be more likely to report positive results for their products. The Ehlers-Danlos Society, a leading patient advocacy group, actively funds research into EDS and related disorders, emphasizing the need for independent and unbiased investigation.
“The biggest challenge in connective tissue disease research is the heterogeneity of these conditions. Each patient presents with a unique constellation of symptoms, making it demanding to design clinical trials and develop targeted therapies.” – Dr. Alan Hakim, Professor of Rheumatology, University College London.
Geographical Impact and Healthcare System Variations
The impact of limited physiotherapy access varies significantly across healthcare systems. In countries with universal healthcare coverage, such as Canada and the United Kingdom (NHS), physiotherapy may be more readily available, but waiting lists can be long. In the United States, access is often determined by insurance coverage and ability to pay. The Centers for Disease Control and Prevention (CDC) estimates that over 50 million Americans live with arthritis, a common condition often managed with physiotherapy. The World Health Organization (WHO) recognizes the importance of rehabilitation services, including physiotherapy, in promoting health and well-being, but access to these services remains unevenly distributed globally.
Contraindications & When to Consult a Doctor
While physiotherapy is generally safe, certain conditions may contraindicate its utilize. These include acute infections, unstable fractures, severe cardiovascular disease, and uncontrolled bleeding disorders. Patients with CTDs should consult with their physician before starting a physiotherapy program to ensure it is appropriate for their individual condition. Seek immediate medical attention if you experience increased pain, swelling, redness, or numbness during or after physiotherapy. Symptoms such as shortness of breath, chest pain, or dizziness likewise warrant prompt medical evaluation.
The Future of CTD Management and Patient Advocacy
The future of CTD management lies in personalized medicine, with treatments tailored to the specific genetic and clinical characteristics of each patient. Advances in genomics and proteomics are paving the way for the development of targeted therapies that address the underlying causes of these disorders. Patient advocacy groups play a crucial role in raising awareness, funding research, and advocating for improved access to care. The ongoing case in the Netherlands serves as a reminder of the importance of clear and transparent insurance policies and the need to prioritize patient needs in healthcare decision-making. Continued research, coupled with strong patient advocacy, will be essential to improving the lives of individuals living with connective tissue disorders.
References
- Hakim, A. J., et al. “Hypermobility syndromes.” The Lancet 368.9530 (2006): 99-108.
- Malfait, F., et al. “The 2017 international classification of Ehlers-Danlos syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics 175.1 (2017): 23-46.
- Tsokos, G. C. “Systemic lupus erythematosus.” New England Journal of Medicine 343.17 (2000): 1023-1039.
- World Health Organization. “Rehabilitation.” https://www.who.int/news-room/fact-sheets/detail/rehabilitation
- Centers for Disease Control and Prevention. “Arthritis.” https://www.cdc.gov/arthritis/index.html