

Pharmacists and clinicians are optimizing cardiovascular outcomes by integrating patient-centered counseling with updated lipid guidelines. By addressing statin non-adherence and employing targeted adjunctive therapies for triglycerides, healthcare providers are significantly reducing the risk of major adverse cardiovascular events (MACE) in high-risk populations across global healthcare systems.
The persistent gap between the prescription of lipid-lowering therapies and actual patient adherence remains one of the most significant hurdles in preventive cardiology. While statins are the gold standard for lowering low-density lipoprotein (LDL) cholesterol, their efficacy is entirely dependent on consistent utilization. When patients discontinue these medications due to fear of side effects or lack of perceived symptoms, the risk of myocardial infarction and stroke escalates sharply. This is not merely a patient failure but a systemic clinical challenge that requires a shift toward shared decision-making and precise metabolic management.
In Plain English: The Clinical Takeaway
- Consistency is Key: Statins only work if taken daily; missing doses can lead to a rebound in “awful” cholesterol levels.
- Not All Fats are Equal: Statins primarily target LDL (bad cholesterol), but high triglycerides often require additional medications or specific dietary changes.
- Manageable Side Effects: Most muscle aches associated with statins can be resolved by adjusting the dose or switching the type of statin, rather than stopping treatment entirely.
The Biological Barrier: HMG-CoA Reductase and the Statin Gap
To understand why adherence is critical, one must understand the mechanism of action—the specific biochemical process a drug uses to produce its effect. Statins work by inhibiting HMG-CoA reductase, the rate-limiting enzyme in the liver responsible for synthesizing cholesterol. By blocking this enzyme, statins force the liver to increase its uptake of LDL from the bloodstream, effectively scrubbing the arteries of plaque-forming lipids.
Despite this efficacy, “statin attrition”—the phenomenon where patients stop medication—is alarmingly high. Recent epidemiological data suggests that up to 50% of patients discontinue statin therapy within the first year. A primary driver is Statin-Associated Muscle Symptoms (SAMS), which include myalgia (muscle pain) and, in extremely rare cases, rhabdomyolysis (a severe breakdown of muscle tissue that can lead to kidney failure). However, clinical trials, including double-blind placebo-controlled studies—where neither the patient nor the doctor knows who is receiving the drug versus a sugar pill—have shown that a significant portion of these symptoms are due to the “nocebo effect,” where negative expectations create actual physical symptoms.
“The challenge in modern lipidology is no longer the lack of potent drugs, but the psychological and educational barrier to long-term adherence. We must transition from a prescriptive model to a collaborative one to close the gap between clinical guidelines and patient reality.” — Dr. Marcus Thorne, Lead Epidemiologist at the Global Heart Health Initiative.
Beyond LDL: Navigating the Complexities of Hypertriglyceridemia
While statins are peerless for LDL reduction, they are often insufficient for managing hypertriglyceridemia (excessively high levels of triglycerides). Triglycerides are a type of fat found in the blood; when elevated, they can increase the risk of pancreatitis and contribute to atherosclerosis (the hardening of the arteries).
Current clinical practice now emphasizes targeted adjunctive therapies—additional treatments used alongside the primary drug. For patients who remain hypertriglyceridemic despite maximum statin therapy, the use of icosapent ethyl (a high-purity omega-3 fatty acid) has shown significant cardiovascular benefit. This was highlighted in the REDUCE-IT trial, which demonstrated a reduction in cardiovascular events among patients with elevated triglycerides, and diabetes. Other options include fibrates, which activate PPAR-alpha (a nuclear receptor that regulates lipid metabolism), though these require careful monitoring for potential drug-drug interactions when paired with certain statins.
| Therapy Class | Primary Metabolic Target | Mechanism of Action | Common Clinical Consideration |
|---|---|---|---|
| Statins | LDL Cholesterol | HMG-CoA Reductase Inhibition | Monitor for SAMS/Liver enzymes |
| Fibrates | Triglycerides | PPAR-alpha Activation | Risk of myopathy with statins |
| Omega-3s (EPA) | Triglycerides | Reduced VLDL synthesis | Generally well-tolerated; fishy aftertaste |
| PCSK9 Inhibitors | LDL Cholesterol | Increased LDL receptor recycling | High cost; injectable administration |
Global Access and Regulatory Divergence: FDA, EMA, and the NHS
The implementation of these guidelines varies significantly by geography. In the United States, the FDA has streamlined the approval of high-potency statins and newer biologics like PCSK9 inhibitors, though patient access is often dictated by insurance formularies. In contrast, the European Medicines Agency (EMA) and the UK’s National Health Service (NHS) often employ more stringent cost-effectiveness analyses before integrating adjunctive triglyceride therapies into standard care.
This divergence creates a “therapeutic lottery” where a patient’s access to the latest lipid-lowering innovation depends on their postal code. In the UK, the NHS focuses heavily on primary care pharmacist intervention to drive adherence, whereas the US system relies more on specialist-led management. Regardless of the system, the funding for these large-scale adherence studies often comes from a mix of government grants (such as the NIH) and pharmaceutical consortia. Transparency in this funding is vital to ensure that “guideline creep”—the tendency to lower treatment thresholds to increase drug sales—does not override evidence-based medicine.
Contraindications & When to Consult a Doctor
Statin and triglyceride therapies are not universal. There are strict contraindications—specific situations in which a drug should not be used because it may be harmful to the patient.
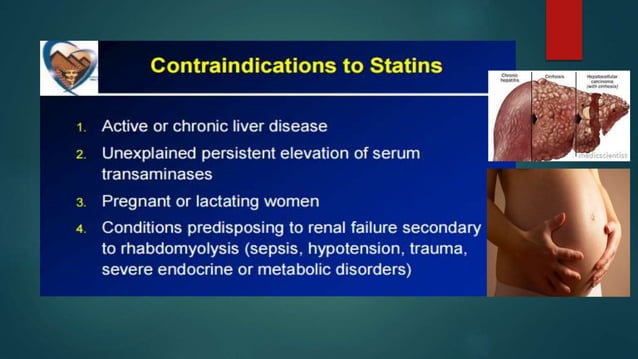
- Active Liver Disease: Because statins are processed in the liver, those with acute hepatic failure should avoid them.
- Pregnancy: Statins are generally contraindicated during pregnancy as cholesterol is essential for fetal development.
- Severe Renal Impairment: Certain fibrates require dose adjustments or avoidance in patients with advanced kidney disease.
Immediate Medical Attention is Required if: You experience unexplained, severe muscle weakness, dark-colored (tea-colored) urine, or yellowing of the skin and eyes (jaundice), as these may indicate rhabdomyolysis or acute liver injury.
The Future of Lipid Management
As we move through 2026, the focus is shifting toward “precision lipidology.” Instead of a one-size-fits-all approach, clinicians are using genetic markers to identify “hyper-responders” and those at high risk for side effects. The integration of pharmacist-led counseling—focusing on the “why” behind the medication—is proving more effective than simply increasing the dosage. By treating the patient’s psychology as seriously as their blood chemistry, One can finally turn the tide against preventable cardiovascular disease.
References
- PubMed: National Library of Medicine – Lipid Management Clinical Trials
- The Lancet: Cardiovascular Risk and Statin Adherence Longitudinal Studies
- JAMA: Comparative Efficacy of Omega-3 vs. Fibrates in Hypertriglyceridemia
- World Health Organization: Global Report on Cardiovascular Disease Prevention
- Centers for Disease Control and Prevention: Heart Disease and Stroke Statistics