
A recent clinical report highlights a diagnostic challenge where a patient with end-stage heart failure and cocaine toxicity suffered a Pulseless Electrical Activity (PEA) arrest. The discovery of a subsequent cerebellar infarction underscores the critical demand for rigorous neurological screening following cardiac resuscitation in high-risk toxicology patients.
For clinicians and public health officials, this case is more than a medical curiosity; it is a cautionary tale regarding the “diagnostic pitfall” of post-resuscitation care. When end-stage heart failure is complicated by stimulant use, the heart’s electrical system may appear functional while the physical pump has failed entirely. This disconnect, combined with the high risk of ischemic strokes—where blood flow to the brain is blocked—creates a complex clinical picture that can easily mislead providers during the golden hour of recovery.
In Plain English: The Clinical Takeaway
- PEA Arrest: This is a state where the heart’s electrical “wiring” is still sending signals, but the muscle is too damaged or weak to actually pump blood.
- Cocaine Cardiotoxicity: Cocaine acts as a sympathomimetic (meaning it mimics the “fight or flight” response), causing the heart to work too hard while simultaneously narrowing the arteries that feed it.
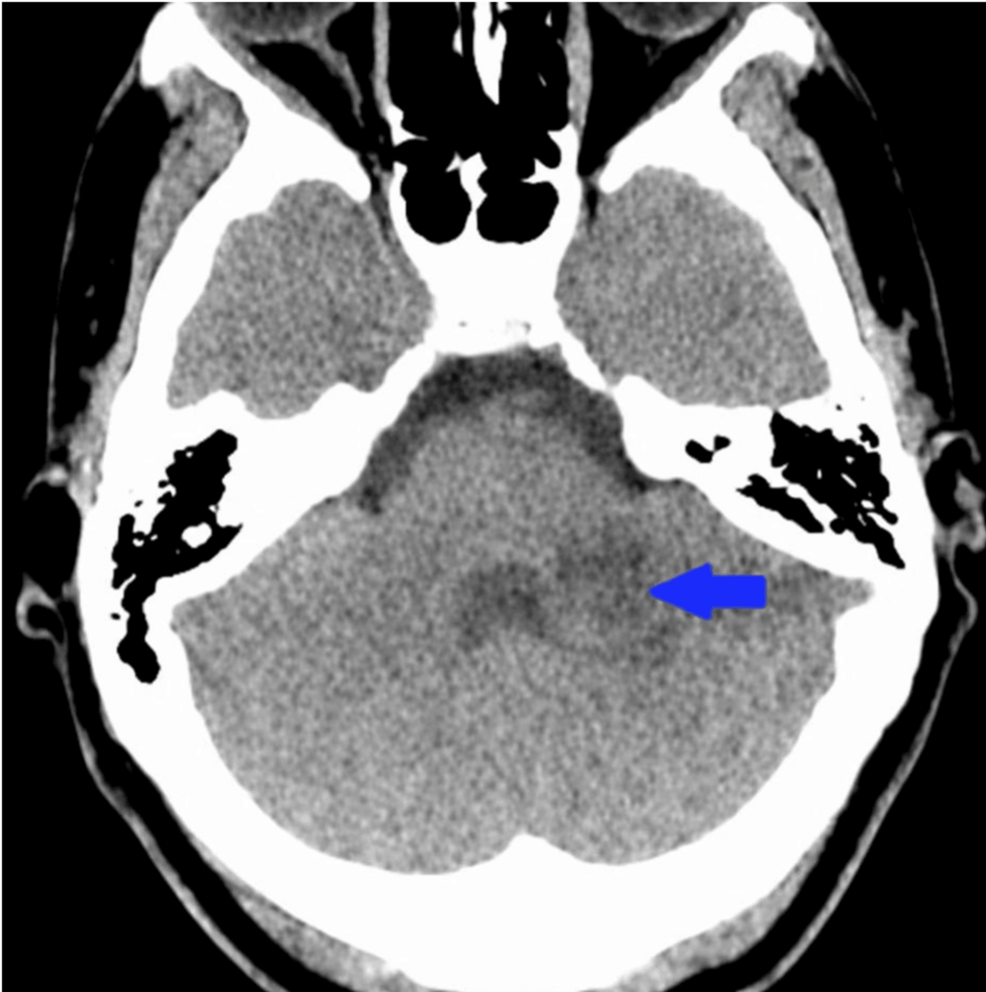
- The Hidden Stroke: A cerebellar infarction is a stroke in the back of the brain. In patients who have suffered cardiac arrest, these can be missed because the patient is often unconscious or sedated.
The Sympathomimetic Surge: How Cocaine Destroys the Myocardium
To understand this arrest, we must examine the mechanism of action—the specific biochemical process—of cocaine on the cardiovascular system. Cocaine blocks the reuptake of norepinephrine, dopamine, and serotonin. This leads to a massive catecholamine surge, which essentially floods the heart with “stress hormones.”

This surge triggers intense vasoconstriction, or the narrowing of blood vessels. In a patient already suffering from end-stage heart failure, the myocardium (the heart muscle) is already starved for oxygen. The addition of cocaine-induced vasoconstriction creates a lethal synergy, leading to myocardial ischemia—a condition where the heart muscle dies due to lack of blood flow.
The result is often Pulseless Electrical Activity (PEA). In PEA, the electrocardiogram (ECG) may show a rhythm that looks “normal” or near-normal, but the ventricles are not contracting. This is a devastating diagnostic trap; the clinician sees electrical activity and may assume the heart is beating, while the patient remains in systemic circulatory collapse.
The Neurological Blind Spot: Cerebellar Infarction Post-Resuscitation
The “diagnostic pitfall” mentioned in the research refers to the neurological aftermath of the arrest. During a PEA event, the brain suffers from global hypoxia—a total lack of oxygen. However, the report emphasizes a specific focal injury: a cerebellar infarction.
The cerebellum coordinates voluntary movements and balance. When a patient is resuscitated from a cardiac arrest, they are often placed in a medically induced coma or are severely encephalopathic (suffering from brain dysfunction). This masks the symptoms of a stroke. If clinicians only focus on the heart, they may miss the window to treat the brain.
“The intersection of stimulant-induced cardiac collapse and post-cardiac arrest syndrome requires a shift in triage. We cannot assume that a successful return of spontaneous circulation (ROSC) equals neurological stability, especially in the presence of cardiotoxic agents.” — Consensus viewpoint aligned with American Heart Association (AHA) post-resuscitation guidelines.
From a geo-epidemiological perspective, this is a growing crisis in North America and Europe. In the United States, the CDC has noted a rise in “polysubstance” use, where stimulants are mixed with opioids. This complicates the clinical presentation, as the respiratory depression of opioids masks the tachycardia (fast heart rate) of cocaine, making the eventual PEA arrest even more sudden and unexpected.
Clinical Comparison: Standard Heart Failure vs. Cocaine-Induced Toxicity
| Clinical Feature | End-Stage Heart Failure (Standard) | Cocaine-Associated Cardiotoxicity |
|---|---|---|
| Primary Mechanism | Chronic remodeling/pump failure | Acute vasoconstriction & catecholamine surge |
| ECG Presentation | Often shows LV hypertrophy or bundle branch blocks | Tachycardia, ST-segment elevation, or PEA |
| Neurological Risk | Chronic hypoperfusion (dementia/fog) | Acute ischemic stroke/cerebellar infarction |
| Primary Treatment | Diuretics, ACE inhibitors, Transplant | Benzodiazepines, Supportive care, Vasodilators |
Funding, Bias, and Systematic Transparency
The underlying case report published in Cureus is typically authored by practicing clinicians and funded through institutional grants or author-supported means. Because this is a case report rather than a double-blind placebo-controlled trial (a study where neither the patient nor the doctor knows who received the treatment), it does not establish a new gold standard of care. Instead, it serves as “clinical intelligence”—real-world evidence that alerts other physicians to a rare but lethal pattern of injury.
The lack of pharmaceutical funding in this specific report removes the risk of commercial bias, ensuring that the focus remains on diagnostic accuracy rather than the promotion of a specific drug therapy.
Contraindications & When to Consult a Doctor
While this article discusses a critical care scenario, the underlying themes of heart failure and stimulant toxicity apply to a broader population. Individuals with pre-existing cardiovascular conditions must be aware of the extreme risks associated with sympathomimetic substances.
Seek emergency medical intervention immediately if you or a loved one experience:
- Sudden onset of ataxia: Loss of coordination or balance (a primary sign of cerebellar dysfunction).
- Crushing chest pain: Especially if accompanied by shortness of breath or radiating pain in the left arm.
- Unresponsive Syncope: Fainting spells that do not resolve quickly.
- Severe Tachycardia: A racing heart that does not slow down during rest.
Contraindication Note: Patients with known heart failure should avoid any stimulants, including high-dose caffeine or over-the-counter decongestants containing pseudoephedrine, as these can mimic the vasoconstrictive effects of cocaine on a weakened heart.
The Path Forward in Post-Resuscitation Care
The trajectory of emergency medicine is moving toward “precision resuscitation.” The lesson from this case is that the heart and brain cannot be treated as separate entities. For patients presenting with stimulant toxicity and cardiac arrest, early neuroimaging (such as CT or MRI) should be prioritized, even if the patient is non-verbal.
By closing the information gap between cardiology and neurology, People can avoid the “diagnostic pitfalls” that turn a successful heart resuscitation into a permanent neurological tragedy.
References
- PubMed Central (National Library of Medicine) – Research on Cocaine-Induced Cardiomyopathy.
- American Heart Association (AHA) – Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.
- Centers for Disease Control and Prevention (CDC) – Data on Stimulant-Related Overdose and Cardiovascular Events.
- The Lancet – Studies on Post-Cardiac Arrest Syndrome and Neurological Outcomes.