

Comorbid personality disorders significantly delay the initiation and success of Obsessive-Compulsive Disorder (OCD) treatment. This clinical overlap often masks core OCD symptoms or hinders a patient’s ability to engage in Exposure and Response Prevention (ERP), leading to prolonged suffering and diminished long-term recovery rates across global healthcare systems.
For decades, the psychiatric community has treated OCD as a primary anxiety-related entity. Still, emerging data discussed in this week’s clinical reviews suggest a more complex interplay. When a patient presents with both OCD and a personality disorder (PD), the diagnostic process is often clouded. The “treatment gap”—the time between the onset of symptoms and the start of evidence-based care—widens because clinicians may misattribute OCD-driven compulsions to the rigid behavioral patterns of a personality disorder, or vice versa.
In Plain English: The Clinical Takeaway
- The Masking Effect: Personality disorders can build OCD symptoms sense like “just part of who I am,” preventing patients from seeking help.
- Therapy Hurdles: The gold-standard treatment for OCD (ERP) is significantly harder to complete when a personality disorder is as well present.
- Integrated Care: Recovery requires a dual-track approach that treats both the OCD and the personality structure simultaneously, rather than sequentially.
The Ego-Syntonic Barrier: Why Personality Disorders Mask OCD
To understand why treatment is delayed, we must examine the distinction between ego-dystonic and ego-syntonic symptoms. OCD is typically ego-dystonic, meaning the thoughts (obsessions) are intrusive, unwanted, and inconsistent with the patient’s self-image. For example, a deeply peaceful person may have intrusive thoughts of violence, which causes immense distress and drives them to seek help.
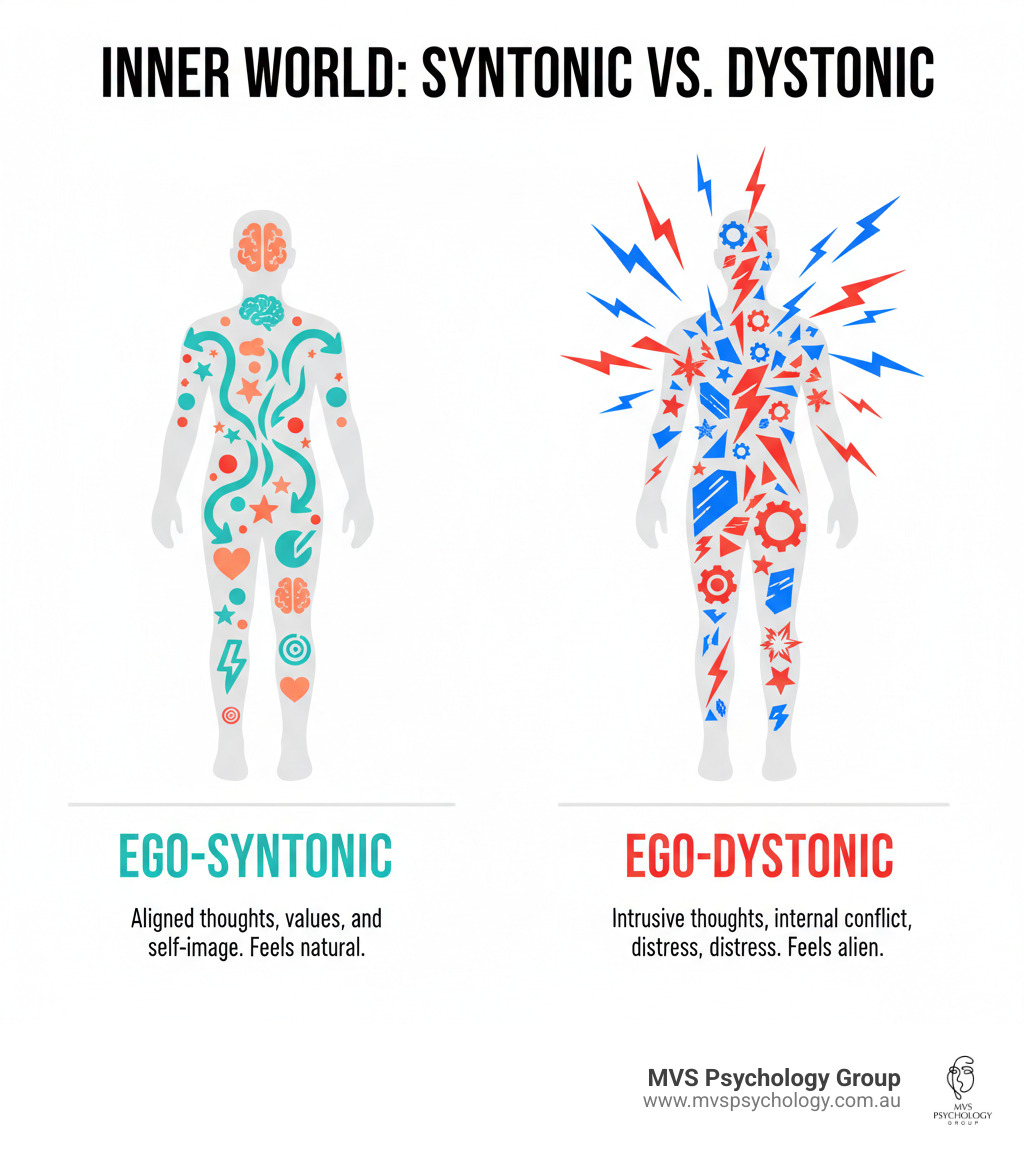
Conversely, personality disorders are often ego-syntonic. This means the behaviors and beliefs are perceived by the patient as natural, correct, or an integral part of their identity. When these two coexist, the ego-syntonic nature of the PD can “absorb” the OCD. A patient with Obsessive-Compulsive Personality Disorder (OCPD)—which is distinct from OCD—may view their rigid adherence to rules not as a distressing compulsion, but as a superior way of living. This reduces the perceived need for clinical intervention, delaying diagnosis by years.
This intersection creates a clinical paradox. While the OCD creates the internal drive for a ritual, the PD provides the justification for it. This synergy often leads to a failure in initial screenings, as the patient may not report the “distress” required for an OCD diagnosis in the ICD-11 (International Classification of Diseases) framework.
The Clinical Friction of ERP in Comorbid Patients
The primary evidence-based treatment for OCD is Exposure and Response Prevention (ERP). This involves exposing the patient to a feared stimulus and preventing the subsequent compulsive response. It is a rigorous process that requires high levels of emotional regulation and therapeutic alliance.
When a Cluster B personality disorder (such as Borderline Personality Disorder) is comorbid, the mechanism of action for ERP is often disrupted. Patients may experience extreme emotional lability—rapid, intense swings in mood—which can lead to premature termination of therapy. The instability in the patient-provider relationship, a hallmark of certain PDs, creates “clinical friction,” where the patient may struggle to trust the therapist’s guidance during the most distressing phases of exposure.
“The challenge in comorbid OCD and personality disorder is not the OCD itself, but the emotional architecture of the patient. If the underlying personality structure is fragmented or highly avoidant, the patient cannot sustain the cognitive load required for successful ERP.” — Dr. Elena Rossi, Lead Researcher in Affective Disorders.
the employ of Selective Serotonin Reuptake Inhibitors (SSRIs), the first-line pharmacological intervention for OCD, may show diminished efficacy or slower response times in patients with severe PDs, necessitating higher dosages or adjunctive antipsychotic medication to stabilize mood before ERP can begin.
Global Healthcare Disparities and the Dual Diagnosis Gap
The impact of this delay varies significantly by geography and healthcare infrastructure. In the United States, the fragmented nature of insurance-based care often separates “personality clinics” from “anxiety clinics,” meaning a patient may be bounced between providers without a cohesive dual-diagnosis plan. This lack of integrated care increases the risk of treatment resistance.
In contrast, the UK’s NHS (National Health Service) utilizes a more centralized referral system, but suffers from extreme wait times for specialized OCD services. When a personality disorder is present, patients are often triaged into general mental health streams rather than specialized OCD tracks, further delaying the application of ERP.
The funding for the underlying research into these comorbidities has largely been driven by university-led grants and national health institutes (such as the NIMH in the US), rather than pharmaceutical funding. This represents critical because there is little profit in “integrated therapy” compared to drug sales, meaning the push for better diagnostic protocols is driven by academic rigor rather than commercial interest.
| Metric | OCD (Standalone) | OCD + Comorbid Personality Disorder |
|---|---|---|
| Avg. Time to Correct Diagnosis | 7–11 Years | 14–18 Years |
| ERP Adherence Rate | High (60-70%) | Moderate to Low (30-40%) |
| Primary Treatment Barrier | Symptom Severity | Emotional Dysregulation/Identity Rigidness |
| Remission Probability (1st Year) | Moderate/High | Low/Moderate |
Contraindications & When to Consult a Doctor
It is imperative to recognize that not all “repetitive behaviors” are OCD. Treating a personality disorder as OCD, or vice versa, can lead to ineffective treatment and increased patient frustration.
Who should avoid self-diagnosis? Individuals experiencing mood swings, chronic instability in relationships, or a lifelong pattern of rigid perfectionism should avoid “DIY” exposure therapy found on social media. Without professional guidance, attempting ERP for complex comorbid cases can lead to severe emotional decompensation or an increase in suicidal ideation.
When to seek immediate professional intervention:
- When compulsions interfere with the ability to maintain employment or basic hygiene.
- When “rituals” are accompanied by intense anger or volatility when interrupted.
- When there is a coexistence of OCD symptoms and a history of self-harm or unstable identity.
- If standard SSRI treatment has failed after 12 weeks of therapeutic dosing.
The Path Toward Integrated Psychiatric Intelligence
The future of treating OCD lies in “transdiagnostic” approaches. Rather than treating the OCD and the personality disorder as two separate enemies, clinicians are moving toward treating the shared underlying vulnerability: cognitive rigidity and emotional dysregulation.
By integrating Dialectical Behavior Therapy (DBT)—which focuses on mindfulness and distress tolerance—with traditional ERP, providers can build the emotional scaffolding necessary for OCD recovery. This shift from a “symptom-first” to a “structure-first” approach is the only way to close the treatment gap and ensure that patients with complex psychiatric profiles are not left behind by a rigid diagnostic system.