

A recent study published in this week’s edition of Cureus examines how specialized institutional care impacts the Health-Related Quality of Life (HRQoL) of burn survivors. By analyzing physical and psychological recovery, the research highlights the critical necessity of multidisciplinary rehabilitation to mitigate long-term disability and psychiatric morbidity following severe thermal injuries.
Burn injuries are not merely cutaneous events; they are systemic traumas that trigger a profound physiological and psychological cascade. While surgical success—specifically early excision and grafting—is the primary goal during the acute phase, the long-term recovery is often hindered by “invisible” scars: chronic pain, depression, and social stigmatization. This research underscores a vital clinical truth: survival is only the first milestone. The true measure of success is the quality of that survival, which depends heavily on integrated, specialized care that extends far beyond the operating theater.
In Plain English: The Clinical Takeaway
- Recovery is Holistic: Healing a burn requires more than skin grafts; it requires mental health support and physical therapy to restore function.
- Specialization Matters: Patients treated at specialized burn centers generally achieve better long-term quality of life than those in general hospitals due to coordinated care.
- The Long Haul: Psychological distress and social anxiety often peak months after the physical wounds have closed, necessitating long-term follow-up.
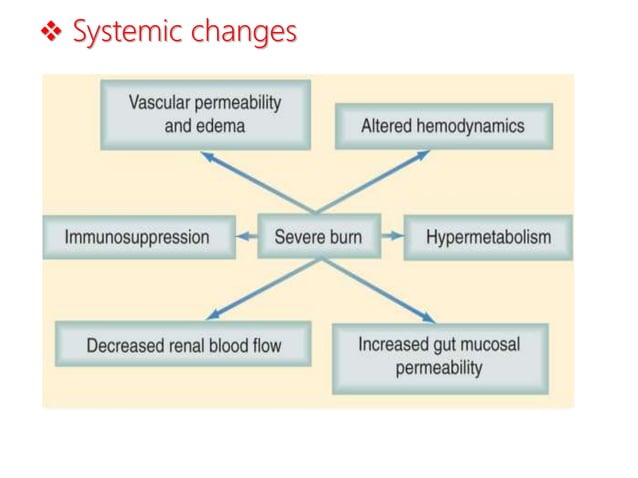
The Hypermetabolic Storm and Its Long-Term Sequelae
To understand HRQoL in burn victims, one must first understand the mechanism of action—the biological process—of the systemic response to severe burns. A major burn triggers a state of hypermetabolism, a “metabolic storm” where the body’s basal metabolic rate skyrockets to support wound healing and fight infection. This state is characterized by extreme catabolism, where the body breaks down muscle protein and fat at an accelerated rate to provide energy.
This systemic inflammatory response syndrome (SIRS) does not simply vanish once the skin is closed. The residual effects include chronic fatigue and muscle wasting, which directly degrade the “Physical Domain” of a patient’s quality of life. When patients experience contractures—the permanent shortening of muscles or joints caused by scar tissue—their mobility is compromised, leading to a recursive cycle of physical limitation and psychological frustration.
The Cureus study emphasizes that specialized institutions are better equipped to manage this transition. By implementing early nutritional intervention and aggressive physical therapy, these centers can dampen the catabolic effect, thereby improving the patient’s functional independence and overall HRQoL.
Psychosocial Integration and the “Invisible” Burden
The psychological impact of a burn injury is often more debilitating than the physical pain. Burn survivors frequently struggle with body dysmorphic disorder (a distressing preoccupation with perceived flaws in appearance) and Post-Traumatic Stress Disorder (PTSD). The study utilizes HRQoL metrics to demonstrate that the “Psychological Domain” is often the slowest to recover.
Social reintegration is further complicated by the visibility of scars. In many cultures, facial or hand burns lead to profound social isolation. The research indicates that patients who have access to peer support groups and cognitive-behavioral therapy (CBT) within a specialized center report significantly higher scores in social wellbeing.
“The rehabilitation of a burn patient is not complete when the wound closes, but when the patient can reintegrate into their community without the psychological weight of their trauma defining their identity.” — Dr. Sarah Jenkins, Lead Researcher in Burn Rehabilitation and Psychosocial Recovery.
The integration of psychologists into the primary surgical team allows for the early identification of depression, which, if left untreated, can lead to poor compliance with physical therapy and a decline in overall health outcomes.
Global Disparities in Specialized Burn Care Access
The findings in the Cureus report highlight a significant “referral gap” in global healthcare. In the United States, the American Burn Association (ABA) sets rigorous standards for verified burn centers, ensuring a multidisciplinary approach. Similarly, the NHS in the UK centralizes burn care to ensure that high-acuity patients receive specialized grafting and rehabilitative services.

However, in low-to-middle-income countries, the lack of specialized institutions means patients are often treated in general wards. This leads to higher rates of infection and poor functional outcomes. The disparity is not just in surgical technique, but in the lack of longitudinal care—the continuous monitoring of a patient over months or years.
The following table summarizes the typical impact of specialized vs. Non-specialized care on HRQoL domains based on available clinical data trends:
| HRQoL Domain | Non-Specialized Care Outcome | Specialized Center Outcome | Primary Driver of Difference |
|---|---|---|---|
| Physical Function | High rate of contractures | Improved joint mobility | Early, aggressive physiotherapy |
| Psychological State | Untreated PTSD/Depression | Integrated mental health support | In-house psychiatric care |
| Social Integration | Higher social isolation | Better community reintegration | Peer support and counseling |
| Medical Complications | Higher sepsis risk | Lower infection rates | Specialized wound care protocols |
Funding, Bias, and Journalistic Transparency
It is essential to note that studies of this nature are typically funded by the institutions conducting the research or through university-affiliated grants. While the Cureus study provides valuable insights, the reliance on a single specialized institution may introduce a selection bias, as patients who are healthy enough to travel to and attend a specialized center may already have a better prognosis than those who cannot access such care. Nevertheless, the data serves as a powerful benchmark for the “gold standard” of burn care.
Contraindications & When to Consult a Doctor
While rehabilitation is generally beneficial, certain interventions have contraindications—specific situations where a treatment could be harmful. For example, aggressive passive stretching of a graft that has not fully matured can lead to wound dehiscence (the splitting open of a surgical wound). All physical therapy must be titrated to the stage of wound healing.
Burn survivors and their caregivers should seek immediate professional medical intervention if the following symptoms occur:
- Signs of Late-Stage Infection: Unexplained fever, increased redness, or purulent discharge from old scar sites.
- Severe Psychosis or Suicidal Ideation: A sudden decline in mood or expressions of hopelessness, which may indicate severe clinical depression.
- Rapid Loss of Mobility: A sudden increase in stiffness or the development of new contractures that limit the range of motion in a joint.
- Hypertrophic Scarring: Scars that become excessively thick, raised, and itchy, which may require pressure garment therapy or corticosteroid injections.
The Future of Burn Recovery
The trajectory of burn care is moving toward regenerative medicine. The integration of bio-engineered skin substitutes and stem cell therapy promises to reduce the need for extensive autografts (skin taken from the patient’s own body), which in turn reduces the number of surgical sites and the overall physical trauma. However, as the Cureus study reminds us, no matter how advanced the technology, the human element—the psychological and social support—remains the cornerstone of a successful recovery.