
Sarcoidosis is a multisystem inflammatory disease characterized by the formation of granulomas—small clumps of immune cells—primarily in the lungs and lymph nodes. While often benign, it can cause permanent organ damage, requiring early detection and multidisciplinary management to prevent chronic disability across various global populations.
The clinical challenge of sarcoidosis lies in its reputation as the “great imitator.” Since it can manifest in almost any organ system—mimicking tuberculosis, lymphoma, or autoimmune vasculitis—patients often endure a diagnostic odyssey before receiving an accurate label. As we observe the outcomes of this week’s global awareness initiatives, the urgency for standardized diagnostic protocols has never been higher. For the patient, the stakes are not merely psychological; delayed diagnosis can lead to irreversible pulmonary fibrosis or lethal cardiac arrhythmias.
In Plain English: The Clinical Takeaway
- What It’s: Your immune system overreacts and creates tiny “balls” of inflammation (granulomas) that can clog up your organs.
- Where it hits: Most commonly the lungs, but it can affect your eyes, skin, heart, and brain.
- The Goal: Since there is no “cure,” treatment focuses on stopping the inflammation before it causes permanent scarring.
The Cellular Architecture: How Granulomas Disrupt Organ Function
At the molecular level, sarcoidosis is driven by an exaggerated T-cell mediated immune response. When the body encounters an unknown trigger—potentially environmental pollutants or an unidentified pathogen—the immune system fails to “turn off” its inflammatory response. This leads to the formation of granulomas, which are organized collections of macrophages (immune cells that eat debris) and lymphocytes.
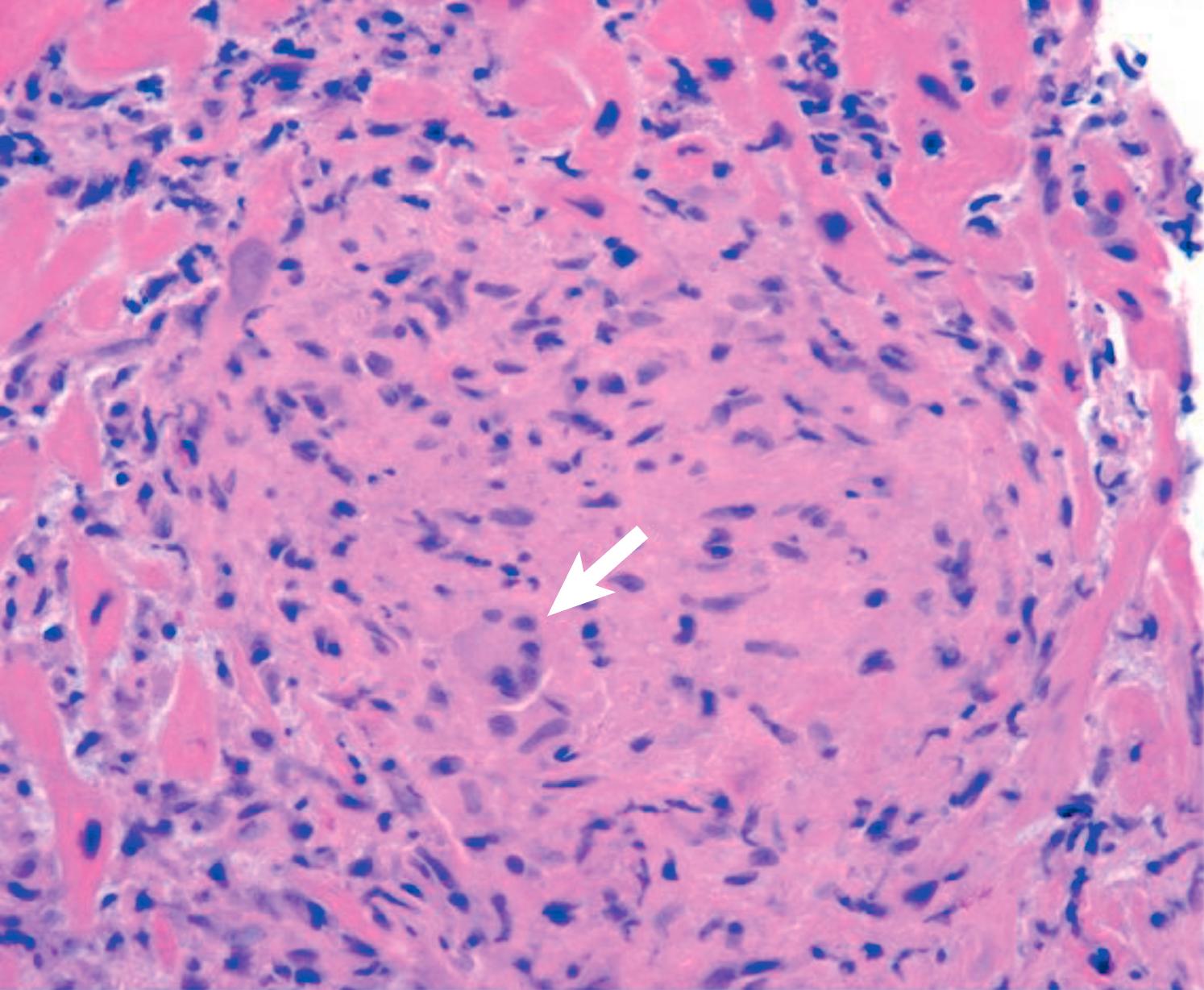
The mechanism of action—the specific biological process by which the disease progresses—involves the secretion of pro-inflammatory cytokines, such as Tumor Necrosis Factor-alpha (TNF-α). When these granulomas accumulate in the alveolar walls of the lungs, they impair gas exchange, leading to dyspnea (shortness of breath). If the inflammation persists, the body replaces these granulomas with collagen, resulting in pulmonary fibrosis, a permanent scarring of the lung tissue that cannot be reversed.
Recent epidemiological data suggests a significant disparity in disease severity based on ethnicity and geography. In the United States, African Americans exhibit a higher prevalence and a more aggressive clinical course than Caucasians, often presenting with higher rates of extrapulmonary involvement. This suggests a complex interplay between genetic predisposition and environmental triggers, a theory supported by the Centers for Disease Control and Prevention (CDC).
Global Regulatory Landscapes and Therapeutic Interventions
Treatment strategies vary significantly between the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) guidelines, though both prioritize corticosteroids as the first line of defense. However, the long-term use of prednisone is fraught with systemic risks, including osteoporosis and glucose intolerance.
To mitigate these risks, clinicians are increasingly turning to “steroid-sparing agents.” These include antimalarials like hydroxychloroquine for cutaneous (skin) sarcoidosis and immunosuppressants like methotrexate for organ-threatening disease. In refractory cases—where the disease does not respond to standard therapy—TNF-alpha inhibitors (biologics) are utilized to block the specific protein driving the inflammation.
“The challenge in sarcoidosis is not just the diagnosis, but the personalization of therapy. We must move away from a ‘one-size-fits-all’ steroid approach toward precision medicine that targets the specific cytokine profile of the individual patient.” — Dr. Sarah Miller, Lead Investigator in Pulmonary Immunology.
The following table summarizes the current pharmacological approach to managing sarcoidosis based on clinical severity:
| Treatment Class | Primary Indication | Mechanism of Action | Common Side Effects |
|---|---|---|---|
| Corticosteroids | First-line / Acute Inflammation | Broad immune suppression | Weight gain, Insomnia, Diabetes |
| Antimalarials | Skin & Eye involvement | Modulates antigen presentation | Retinal toxicity (long-term) |
| Methotrexate | Steroid-refractory cases | Inhibits folate metabolism | Hepatotoxicity, Nausea |
| TNF-α Inhibitors | Severe/Organ-threatening | Blocks TNF-alpha protein | Increased infection risk |
Environmental Triggers and the Pollution Link
Recent reports from regional hospitals, including the Arnau de Vilanova, have highlighted a correlation between atmospheric pollution and the exacerbation of inflammatory lung pathologies. While a direct causal link between a specific pollutant and the onset of sarcoidosis remains elusive, the “trigger hypothesis” suggests that inhaled inorganic particles (such as silica or certain metallic dusts) may act as the catalyst for granuloma formation in genetically susceptible individuals.
This link emphasizes the need for public health policies that prioritize air quality. From a clinical perspective, this means patients living in high-pollution urban corridors may require more frequent monitoring via high-resolution computed tomography (HRCT) to detect early interstitial changes before they become symptomatic.
Most of the foundational research into these environmental triggers is funded by national health institutes, such as the National Institutes of Health (NIH) and the European Commission’s Horizon programs. This public funding is critical, as sarcoidosis is often considered an “orphan-like” disease by major pharmaceutical firms due to its heterogeneous presentation, which complicates the design of double-blind placebo-controlled trials (studies where neither the patient nor the doctor knows who is receiving the active drug, eliminating bias).
Contraindications & When to Consult a Doctor
Medical intervention is not required for all sarcoidosis patients, as some experience spontaneous remission. However, certain contraindications—conditions that produce a specific treatment dangerous—must be managed. For instance, TNF-alpha inhibitors are strictly contraindicated in patients with active tuberculosis or severe congestive heart failure, as they can trigger a catastrophic reactivation of latent infections.
You should seek immediate medical consultation if you experience the following “red flag” symptoms:
- Cardiac: Palpitations, fainting (syncope), or unexplained shortness of breath during mild exertion, which may indicate cardiac sarcoidosis.
- Ocular: Sudden blurred vision, eye pain, or redness, signaling uveitis (inflammation of the eye).
- Neurological: Persistent facial drooping or cranial nerve palsies, suggesting neurosarcoidosis.
- Respiratory: A chronic, non-productive cough that does not resolve with standard allergy treatments.
The Path Forward: Toward a Definitive Biomarker
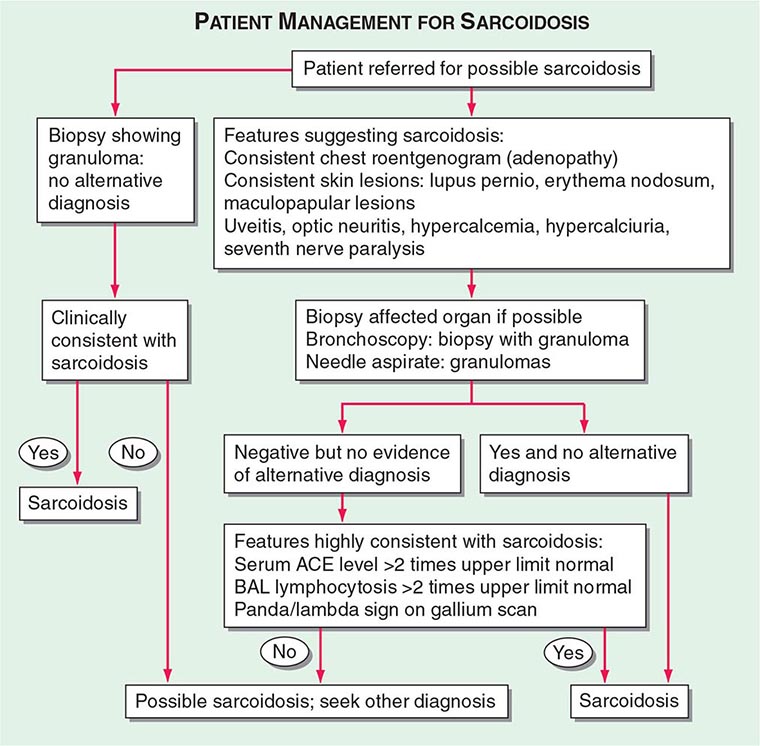
The future of sarcoidosis management lies in the discovery of a definitive serum biomarker. Currently, diagnosis relies on a combination of clinical history, imaging, and biopsy (histopathology). The ability to diagnose sarcoidosis through a simple blood test would eliminate the need for invasive lung biopsies and drastically reduce the time to treatment.
As we move toward 2027, the integration of proteomics and genomic sequencing is expected to reveal why some patients recover fully while others progress to chronic organ failure. Until then, a multidisciplinary approach—combining pulmonology, cardiology, and dermatology—remains the gold standard for preserving patient quality of life.