

Recent longitudinal analyses confirm that high fluid intake combined with dietary calcium and sodium regulation significantly reduces nephrolithiasis risk. This evidence-based protocol addresses the rising prevalence affecting one in 10 Americans. Patients should prioritize hydration and consult providers before altering supplement regimens to ensure safety.
The prevalence of kidney stones, clinically known as nephrolithiasis, is not merely a statistical anomaly; it is a growing public health crisis. As of this spring, epidemiological data indicates a persistent upward trajectory in incidence rates across North America and Europe. For patients, this translates to increased emergency department visits, higher healthcare costs, and significant physical morbidity. Understanding the specific combination of preventive factors is no longer optional wellness advice; it is critical clinical intelligence. This report synthesizes current consensus to separate actionable physiology from social media fiction.
The Metabolic Architecture of Stone Formation
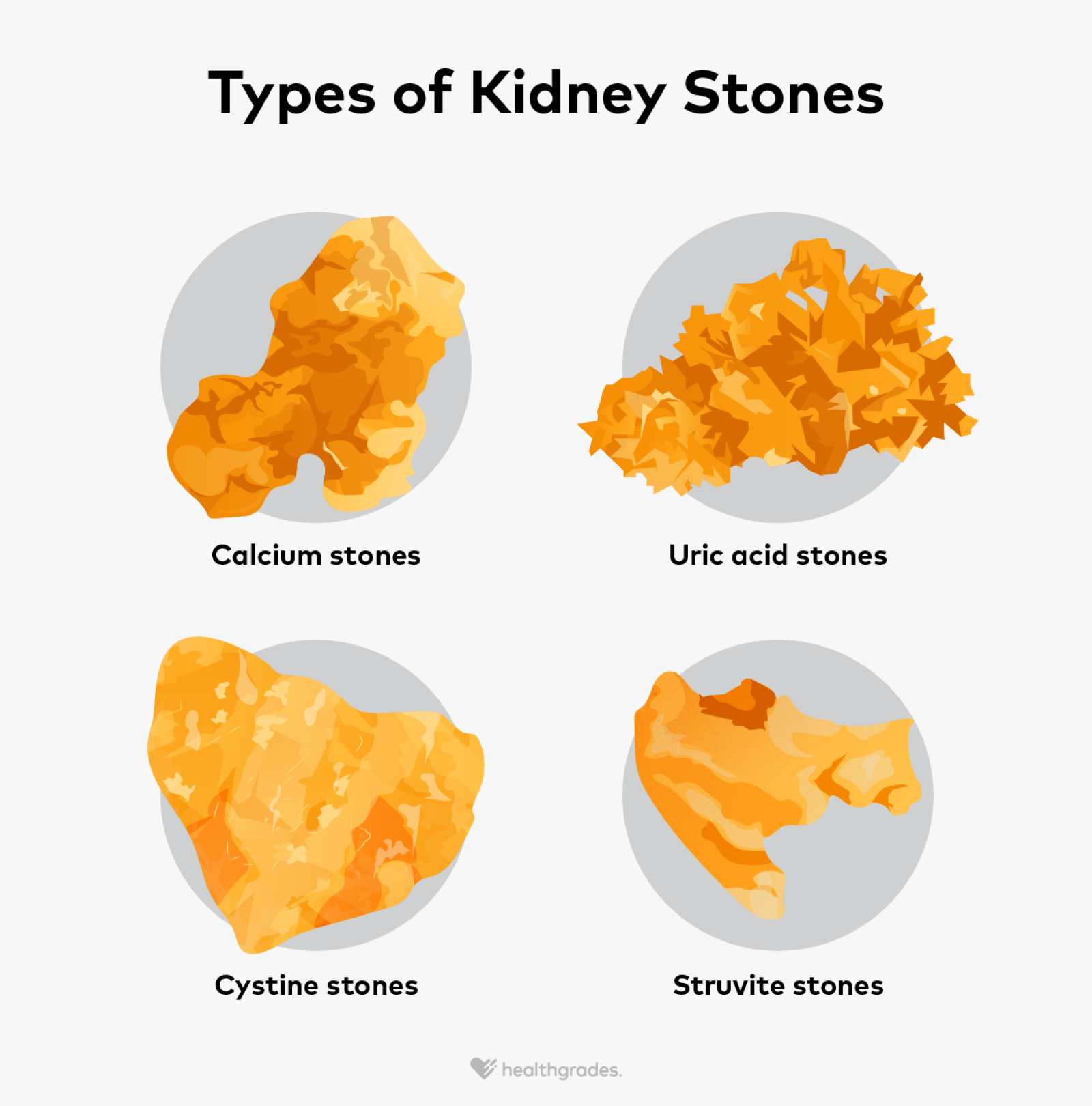
To understand prevention, one must understand the mechanism of action. Kidney stones form when urine becomes supersaturated with crystal-forming substances such as calcium, oxalate, and uric acid. Under normal physiological conditions, urine contains inhibitors that prevent these crystals from binding together. However, when fluid volume is insufficient, or when dietary drivers elevate urinary excretion of stone-forming salts, crystallization occurs.
Recent data reinforces that calcium restriction is often counterproductive. Dietary calcium binds to oxalate in the gastrointestinal tract, preventing its absorption into the bloodstream and subsequent excretion through the kidneys. Conversely, calcium supplements taken without food may increase risk. This distinction highlights the importance of source over simple quantity. Sodium intake directly influences calcium excretion; high sodium levels force the kidneys to excrete more calcium, thereby increasing the substrate available for stone formation.
In Plain English: The Clinical Takeaway
- Hydration is Primary: Drinking enough water to produce at least 2.5 liters of urine daily dilutes stone-forming salts.
- Eat Calcium, Don’t Supplement Blindly: Consume calcium-rich foods with meals to bind oxalate in the gut rather than taking isolated pills.
- Limit Sodium: Reducing salt intake lowers the amount of calcium your kidneys must filter, directly reducing stone risk.
Geographic Disparities and Regulatory Frameworks
The burden of nephrolithiasis is not distributed equally. In the United States, the “Stone Belt” in the southern and eastern regions shows higher incidence, likely due to climate-induced dehydration and dietary patterns. Regulatory bodies like the FDA monitor dietary supplements closely, yet over-the-counter vitamin formulations remain a common vector for excessive intake. In contrast, the NHS in the United Kingdom emphasizes primary care prevention protocols to reduce surgical intervention rates.
Access to metabolic testing varies by region. In the US, 24-hour urine collection is the gold standard for high-risk patients but is underutilized in primary care settings. International guidelines from the European Association of Urology align closely with American Urological Association (AUA) standards, emphasizing that prevention is a systemic metabolic management issue rather than a singular dietary fix.
“Dietary modification remains the cornerstone of prevention. We must move patients away from empiric restriction and toward personalized metabolic evaluation to reduce recurrence rates effectively.”
This consensus statement reflects the stance of major urological bodies regarding the necessity of personalized care plans. Funding for large-scale cohort studies often comes from national institutes such as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Transparency in this funding is vital, as it ensures that recommendations prioritize patient outcomes over commercial supplement interests.
| Risk Factor | Physiological Impact | Preventive Action |
|---|---|---|
| Low Fluid Intake | Increases urine supersaturation | Target 2.5L urine output/day |
| High Sodium Diet | Increases urinary calcium excretion | Limit to <2,300 mg/day |
| Low Dietary Calcium | Increases oxalate absorption | Consume 1,000-1,200 mg/day with meals |
| High Animal Protein | Lowers urinary citrate, increases acid | Moderate intake, increase plant proteins |
Funding Transparency and Research Trajectory
Research into nephrolithiasis prevention is predominantly funded by public health institutions and academic medical centers. This public funding model reduces the risk of commercial bias often seen in supplement-driven nutrition studies. Current longitudinal studies are focusing on the genetic predispositions that interact with environmental factors. As we move through 2026, the integration of genetic profiling into standard urological care may allow for even more precise dietary prescriptions.
However, patients must remain wary of unverified claims regarding “alkalizing” diets or miracle supplements. The mechanism of action for citrate therapy, for example, is well-understood: it binds to calcium in the urine, preventing crystal growth. This is a pharmacological effect achieved through medication or specific dietary intake, not a vague wellness trend. Objective statistical probability shows that adherence to established medical guidelines reduces recurrence by significant margins compared to anecdotal remedies.
Contraindications & When to Consult a Doctor
While dietary modification is generally safe, specific contraindications exist. Patients with chronic kidney disease (CKD) must manage fluid and electrolyte intake under strict supervision to avoid volume overload or hyperkalemia. Individuals with a history of calcium phosphate stones may respond differently to urinary alkalinization than those with calcium oxalate stones.
Immediate medical consultation is warranted if you experience severe flank pain, hematuria (blood in urine), or fever accompanied by urinary symptoms. These may indicate an obstructing stone or infection, which are urological emergencies. Do not attempt to treat acute stone passage solely with home remedies. Professional triage ensures that obstruction does not lead to permanent renal damage.
The trajectory of kidney stone prevention is moving toward precision medicine. By combining high-volume hydration with nuanced dietary management, patients can significantly alter their risk profile. This approach requires discipline and medical partnership, but the reduction in pain and healthcare burden is statistically robust. As research evolves, the core tenets of hydration and balanced nutrition remain the most potent tools available.
References
- National Institute of Diabetes and Digestive and Kidney Diseases. Kidney Stones.
- American Urological Association. Medical Management of Kidney Stones Guideline.
- Centers for Disease Control and Prevention. Kidney Disease Information.
- PubMed Central. Peer-Reviewed Literature on Nephrolithiasis.
- National Kidney Foundation. Stone Safety.