

Economic disparity in Spain significantly restricts access to dental care, with high-income adults visiting dentists at a rate 25% higher than low-income peers in 2025. This gap exacerbates systemic health risks, as untreated oral pathologies often correlate with chronic conditions including cardiovascular disease and uncontrolled diabetes.
The divide in oral healthcare is not merely a matter of aesthetics or comfort; It’s a critical failure in the Social Determinants of Health (SDOH)—the non-medical factors, such as income and education, that influence health outcomes. When a significant portion of the population is priced out of preventative dentistry, the result is a shift from proactive maintenance to reactive, emergency intervention. This transition increases the burden on public emergency rooms and elevates the risk of systemic comorbidities.
In Plain English: The Clinical Takeaway
- The Wealth Gap is a Health Gap: People with more money are significantly more likely to get preventative dental check-ups, preventing small problems from becoming surgical emergencies.
- Mouth-Body Connection: Severe gum disease isn’t just about teeth; it can leak bacteria into the bloodstream, increasing the risk of heart attacks and strokes.
- Prevention vs. Crisis: Regular cleaning is affordable and simple, but waiting until a tooth abscesses requires expensive, invasive treatment that low-income patients often cannot afford.
The Oral-Systemic Link: How Financial Barriers Trigger Biological Decay
To understand why a gap in dental visits is a public health crisis, we must examine the mechanism of action—the specific biological process—of periodontal disease. Periodontitis is a chronic inflammatory disease that destroys the supporting structures of the teeth. When left untreated due to financial barriers, the oral cavity becomes a reservoir for pathogenic bacteria such as Porphyromonas gingivalis.
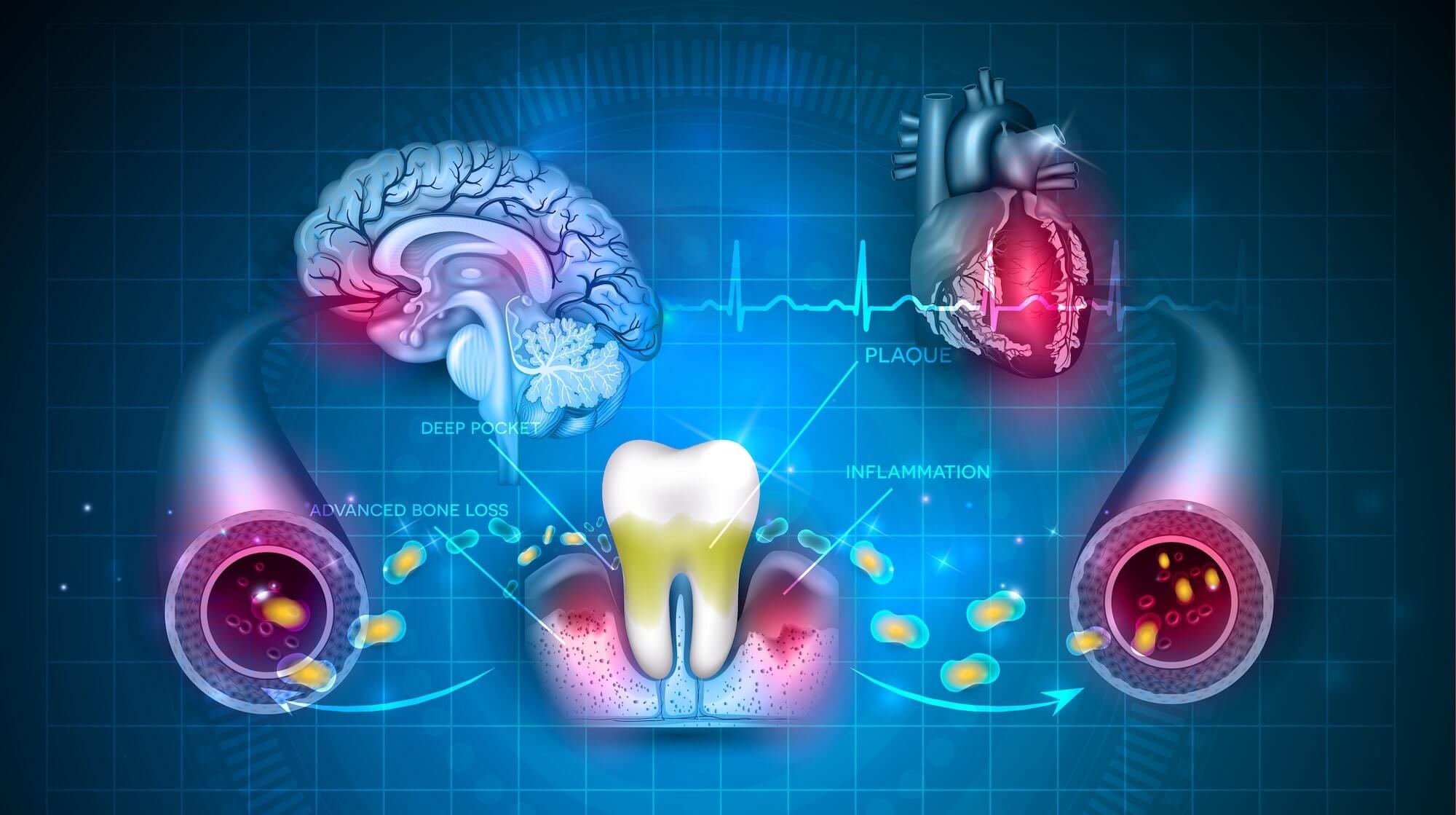
These bacteria can enter the circulatory system, triggering a state of chronic systemic inflammation. This is often measured via C-reactive protein (CRP), a biomarker in the blood that indicates inflammation. High levels of systemic inflammation are closely linked to atherosclerosis (the hardening of arteries) and insulin resistance. Essentially, the inability to afford a dental cleaning can contribute to the progression of cardiovascular disease.
Research published in PubMed suggests that the inflammatory load from chronic periodontitis can exacerbate glycemic control in patients with Type 2 diabetes, creating a bidirectional relationship where the disease in the mouth makes the disease in the blood harder to manage.
Geo-Epidemiological Bridging: Spain’s SNS vs. Global Models
Spain’s Sistema Nacional de Salud (SNS) provides comprehensive primary healthcare, yet dental care remains largely privatized or restricted to specific vulnerable groups and children. This creates a “two-tier” system. While the European Medicines Agency (EMA) regulates the pharmaceuticals used in dental care, it does not regulate the access to the practitioners who administer them.
This mirrors a global trend seen in the UK’s NHS, where “dental deserts” have emerged, leaving low-income populations without local providers. In the United States, the disparity is even more pronounced, often tied to the lack of dental insurance in Medicaid expansions. The Spanish data from 2025 highlights that even within a robust socialized medicine framework, the exclusion of dental health from the universal “basket of services” creates a profound health inequity.
“The persistence of oral health inequalities is a marker of systemic failure. When we treat the mouth as separate from the body, we ignore the physiological reality that oral infections are gateways to systemic chronic diseases.” — Dr. Maria Elena Rodriguez, Epidemiologist specializing in Social Medicine.
Data Analysis: Access Rates and Health Correlations
The following data summarizes the disparity in dental utilization and the associated clinical risks associated with the lack of preventative care observed in recent Spanish population studies.
| Income Bracket | 2025 Dental Visit Rate | Primary Clinical Risk | Long-term Systemic Impact |
|---|---|---|---|
| High Income | 67.4% | Low (Preventative Focus) | Reduced inflammatory markers |
| Low Income | 42.3% | High (Reactive Focus) | Elevated risk of CVD & Diabetes |
| Average Gap | 25.1% | Delayed Diagnosis | Increased ER admissions for sepsis |
This research is primarily derived from the Encuesta Nacional de Salud (National Health Survey), funded by the Spanish Ministry of Health. Because this is government-funded surveillance data, it lacks the commercial bias found in industry-sponsored trials, providing a transparent look at the socioeconomic failures of the current healthcare delivery model.
The Pathological Cost of Delayed Intervention
When patients avoid the dentist due to cost, they enter a cycle of “dental triage.” Instead of a prophylactic cleaning (preventative care), they wait for a symptomatic crisis, such as a periapical abscess—a collection of pus at the root of a tooth. This often leads to emergency department visits for intravenous antibiotics and surgical drainage.
The double-blind placebo-controlled nature of most pharmaceutical trials for oral health drugs often overlooks the “real-world” application in low-income settings. While a drug may be effective in a controlled trial, its efficacy is nullified if the patient cannot afford the prerequisite clinical cleaning required for the medication to work.
Contraindications & When to Consult a Doctor
While preventative care is the goal, certain symptoms indicate an acute medical emergency that overrides financial concerns. Make sure to seek immediate professional intervention if you experience:
- Facial Cellulitis: Swelling of the cheek or jaw that extends toward the eye or neck, which can obstruct the airway.
- Systemic Fever: A high fever accompanying a toothache, suggesting the infection has entered the bloodstream (sepsis).
- Severe Gingival Recession: Gums pulling away from the teeth accompanied by persistent bleeding, which may indicate advanced periodontitis.
- Unexplained Oral Lesions: Any sore or white patch in the mouth that does not heal within 14 days, which requires a biopsy to rule out oral squamous cell carcinoma.
The Trajectory of Public Health Equity
Moving forward, the integration of oral health into primary care is the only evidence-based solution to close this gap. As highlighted by the World Health Organization (WHO), oral health must be repositioned as an integral part of non-communicable disease (NCD) prevention strategies. Without a policy shift in Spain to subsidize preventative dental care for low-income brackets, the economic divide will continue to manifest as a biological divide, shortening the healthy life expectancy of the most vulnerable citizens.
References
- World Health Organization (WHO) – Global Oral Health Status Report.
- The Lancet – Social Determinants of Health and Chronic Disease.
- PubMed – Periodontal Disease and Systemic Inflammation (CRP Markers).
- Spanish Ministry of Health – Encuesta Nacional de Salud 2025.
- Journal of the American Medical Association (JAMA) – Socioeconomic Status and Healthcare Access.