
{kind=link}
The Rising Incidence of Spigelian Hernias Post-Hysterectomy: Predicting a Shift in Surgical Repair Strategies
Nearly 1 in 5 women will undergo a hysterectomy in their lifetime. While often life-changing for the better, the long-term implications of this surgery are increasingly coming into focus, particularly concerning unexpected complications. A recent case report published in Cureus highlights a concerning trend: the emergence of Spigelian hernias following laparoscopic hysterectomy. This isn’t a statistically common occurrence *yet*, but the increasing number of minimally invasive hysterectomies, coupled with evolving understandings of abdominal wall biomechanics, suggests we may see a significant rise in these challenging-to-diagnose hernias. This article explores the factors driving this trend, the potential for improved diagnostic techniques, and the future of surgical repair.
Understanding the Connection: Hysterectomy and Abdominal Wall Integrity
Spigelian hernias occur along the semilunar line – a naturally weaker area of the abdominal wall located laterally to the rectus abdominis muscle. Traditionally, they’ve been associated with straining, obesity, and prior abdominal surgeries. However, the laparoscopic approach to hysterectomy, while offering benefits like reduced pain and faster recovery, introduces unique biomechanical stresses. The manipulation of tissues during laparoscopic procedures, combined with the removal of the uterus’s supporting weight, can subtly compromise the integrity of the abdominal wall, predisposing patients to Spigelian hernia formation. **Spigelian hernia** diagnosis is often delayed due to their atypical presentation and location, making early detection crucial.
“Did you know?” box: Spigelian hernias account for only 1-2% of all abdominal hernias, making them particularly challenging to recognize. Their small size and location often lead to misdiagnosis as other conditions, like musculoskeletal pain or lipomas.
The Role of Minimally Invasive Surgery
Laparoscopic hysterectomy has become the gold standard for many gynecological surgeons. However, the trocar sites used for instrument insertion create points of potential weakness. While these sites are typically closed, subtle fascial defects can develop over time, especially in individuals with pre-existing risk factors. Furthermore, the pneumoperitoneum (inflation of the abdomen with gas) during laparoscopic surgery alters intra-abdominal pressure and can contribute to fascial strain. The increasing prevalence of laparoscopic hysterectomy, therefore, is a key driver in the potential rise of Spigelian hernias.
Future Diagnostic Advancements: Beyond Clinical Examination
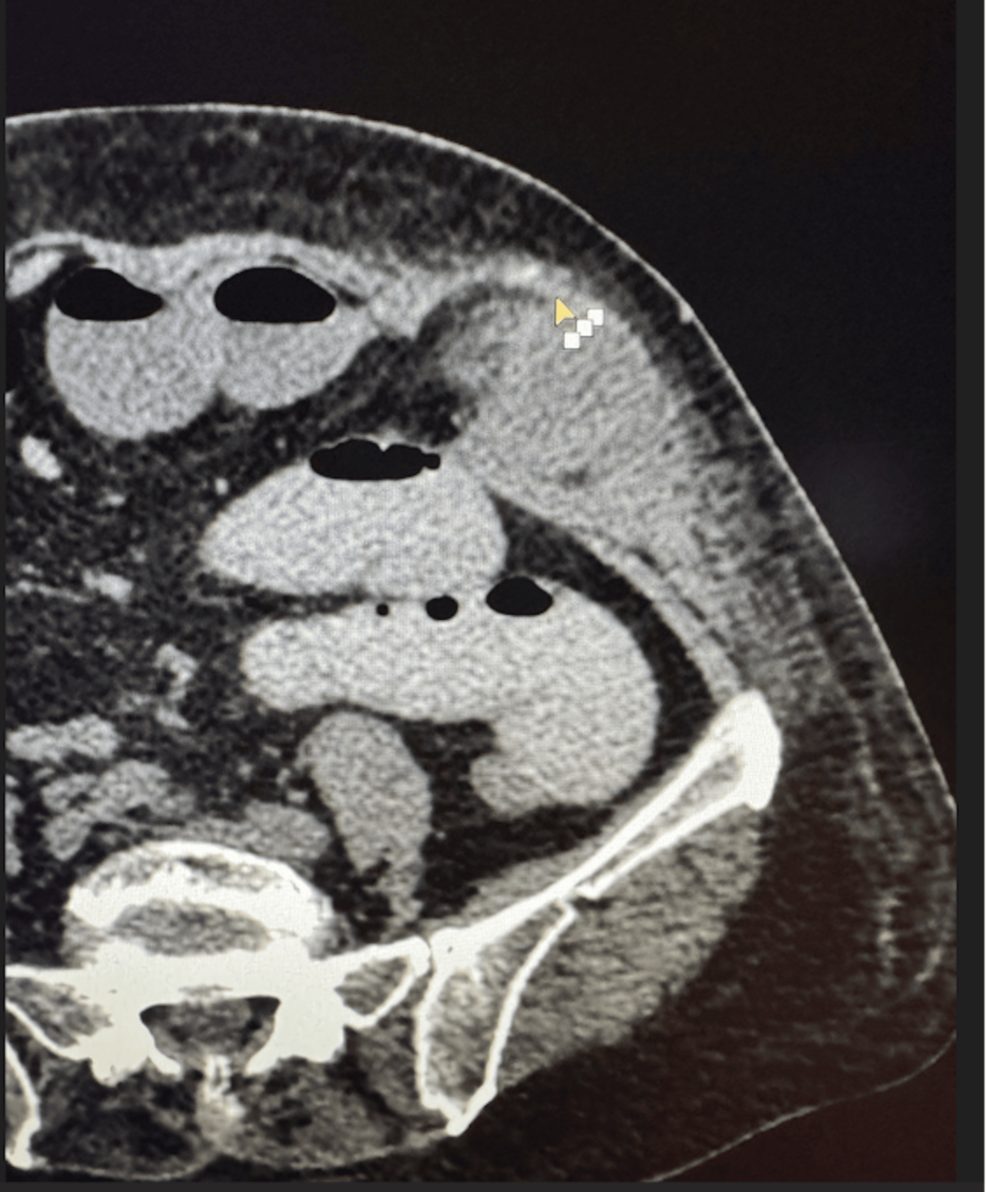
Currently, diagnosing a Spigelian hernia relies heavily on clinical examination, which can be unreliable due to the hernia’s often subtle presentation. Imaging modalities like ultrasound and CT scans can be helpful, but sensitivity and specificity vary. The future of diagnosis likely lies in a combination of improved imaging techniques and a heightened awareness among clinicians.
“Expert Insight:” Dr. Anya Sharma, a leading surgical oncologist, notes, “We need to move beyond relying solely on physical examination. High-resolution ultrasound with experienced sonographers, coupled with a low threshold for CT imaging in suspected cases, will be critical for earlier and more accurate diagnoses.”
Emerging technologies, such as elastography (a technique that measures tissue stiffness), may offer a non-invasive way to assess abdominal wall integrity and identify areas of weakness. Artificial intelligence (AI) algorithms trained on large datasets of imaging studies could also assist in identifying subtle signs of Spigelian hernias that might be missed by the human eye. The integration of these technologies promises a more proactive and precise diagnostic approach.
Surgical Repair: Evolving Techniques and Materials
The surgical repair of Spigelian hernias presents unique challenges due to their location and the often-compromised surrounding tissues. Traditional open repair involves direct suture closure of the fascial defect, but this can be associated with high recurrence rates. Minimally invasive techniques, such as laparoscopic or robotic-assisted repair, are gaining traction, offering potential benefits like reduced pain and faster recovery. However, these techniques require specialized training and expertise.
The choice of mesh material is also a critical consideration. While mesh reinforcement can significantly reduce recurrence rates, concerns about mesh-related complications, such as chronic pain and infection, have led to increased scrutiny. Future research will likely focus on developing biocompatible, bioresorbable meshes that provide adequate support without the long-term risks associated with permanent synthetic materials.
“Pro Tip:” When discussing surgical options with your surgeon, ask about their experience with Spigelian hernia repair and the specific techniques and materials they recommend. Understanding the potential benefits and risks of each approach is crucial for making an informed decision.
Personalized Repair Strategies
A “one-size-fits-all” approach to Spigelian hernia repair is unlikely to be optimal. Factors such as the size and location of the defect, the patient’s age and overall health, and the presence of any co-morbidities should all be considered when developing a personalized repair strategy. The use of biomechanical modeling and finite element analysis could help surgeons predict the stresses on the abdominal wall and tailor the repair accordingly.
The Broader Implications: Abdominal Wall Reconstruction and Preventative Measures
The increasing awareness of Spigelian hernias following hysterectomy highlights the importance of considering abdominal wall integrity in all surgical procedures. Future research should focus on identifying risk factors for abdominal wall compromise and developing preventative measures. This could include optimizing surgical techniques to minimize tissue trauma, using prophylactic mesh reinforcement in high-risk patients, and promoting post-operative rehabilitation programs to strengthen the abdominal muscles.
“Key Takeaway:” The rise in Spigelian hernias post-hysterectomy isn’t just a surgical issue; it’s a signal that we need a more holistic approach to abdominal wall health, encompassing pre-operative risk assessment, meticulous surgical technique, and comprehensive post-operative care.
Frequently Asked Questions
What are the symptoms of a Spigelian hernia?
Symptoms can be vague and include localized pain, a bulge in the lower abdomen, or a feeling of discomfort. However, many Spigelian hernias are asymptomatic and discovered incidentally during imaging for other reasons.
Is surgery always necessary for a Spigelian hernia?
Not always. Small, asymptomatic hernias may be monitored. However, surgery is generally recommended for symptomatic hernias or those at risk of incarceration (where the hernia becomes trapped and blood supply is cut off).
What is the recovery like after Spigelian hernia repair?
Recovery time varies depending on the surgical technique used. Minimally invasive repairs typically have a faster recovery than open repairs. Patients are usually advised to avoid heavy lifting and strenuous activity for several weeks.
Can Spigelian hernias recur after repair?
Yes, recurrence is possible, although the risk can be minimized with appropriate surgical technique and mesh reinforcement. Following your surgeon’s post-operative instructions is crucial for preventing recurrence.
What are your thoughts on the future of abdominal wall surgery? Share your insights in the comments below!