
{kind=link}
Steroids for Vasculitis: A Double-Edged Sword for the Pancreas
Table of Contents
- 1. Steroids for Vasculitis: A Double-Edged Sword for the Pancreas
- 2. Understanding the Link: Vasculitis what alternative immunosuppressants can be considered to minimize steroid use in chronic LCV, and how might they reduce the risk of steroid-induced pancreatitis?
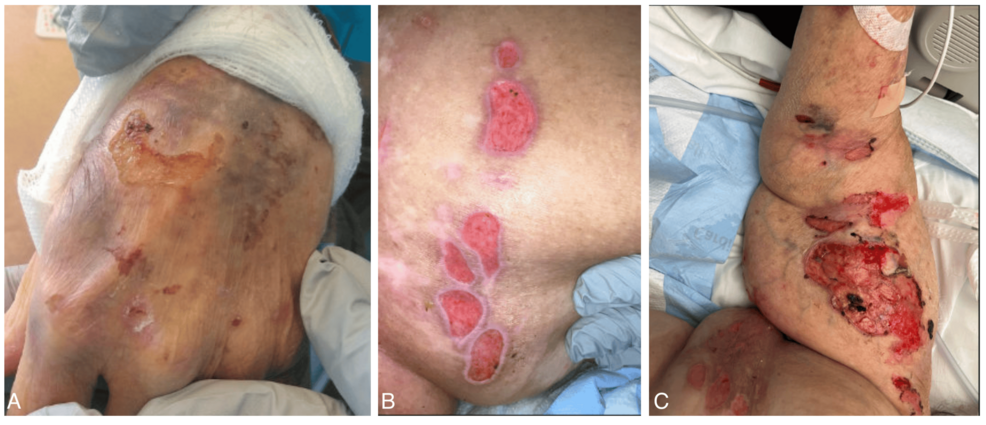
- 3. Steroid-induced Pancreatitis Following leukocytoclastic Vasculitis
- 4. Understanding the Connection: Vasculitis, Steroids, and the Pancreas
- 5. Leukocytoclastic Vasculitis: A Brief overview
- 6. How Steroids Trigger Pancreatitis
- 7. Recognizing Steroid-Induced Pancreatitis: Symptoms & Diagnosis
- 8. Management Strategies: A Multi-Disciplinary Approach
- 9. Proactive prevention: Minimizing Risk in LCV Treatment
For individuals battling leukocytoclastic vasculitis, the road to recovery often involves powerful anti-inflammatory medications, primarily corticosteroids. These drugs are vital in taming the immune system’s inflammatory response.
However, a critical, though less common, complication can arise: steroid-induced pancreatitis. This means the very treatment designed to heal can, in some unfortunate instances, trigger a new and serious health issue.