
New research from NYU Grossman School of Medicine indicates sugary drink taxes fail to reduce calorie purchases in U.S. Fast-food settings. Published in PLOS Medicine, the study suggests fiscal policies alone may not alter consumer behavior in quick-service restaurants. Patients should focus on individual dietary choices rather than relying on regulatory measures for metabolic health protection.
As a physician observing the intersection of public policy and metabolic health, I view this data with critical clarity. While taxation aims to reduce the incidence of type 2 diabetes and obesity by increasing the cost of sugar-sweetened beverages (SSBs), the behavioral economics of fast-food environments appear resistant to price hikes. This matters globally due to the fact that health systems, from the NHS in the UK to private insurers in the US, bank on these policies to lower long-term cardiovascular risk profiles. If the mechanism of action—price elasticity—fails in high-volume settings, we must recalibrate our prevention protocols.
In Plain English: The Clinical Takeaway
- Taxes Don’t Stop Fast-Food Sugar: Adding costs to sugary drinks at drive-throughs does not significantly change what customers order.
- Metabolic Risk Remains: Patients cannot rely on government policies to protect them from high fructose corn syrup; personal selection is key.
- Policy vs. Biology: Public health laws perform better in grocery stores than in fast-food chains where menu options are limited.
The Economic Mechanism Versus Metabolic Reality
The study utilized a difference-in-differences analysis to compare purchase data before and after tax implementation. In clinical terms, think of this as a double-blind placebo-controlled design applied to economics: researchers looked for a signal amidst the noise of consumer habit. The hypothesis was that higher prices would trigger a negative feedback loop, reducing consumption. However, the data suggests that in fast-food ecosystems, the mechanism of action is disrupted by brand loyalty and limited substitution options.
Biologically, the consumption of liquid carbohydrates bypasses normal satiety signals. When a patient consumes high-glycemic beverages, insulin spikes rapidly, often leading to subsequent hypoglycemia and increased hunger. A tax aims to reduce this exposure. However, if the price increase is absorbed by the consumer without changing the order, the physiological burden remains unchanged. This disconnect highlights a limitation in using fiscal tools alone to manage chronic disease vectors like obesity.
Geo-Epidemiological Bridging: US Policy vs. Global Standards
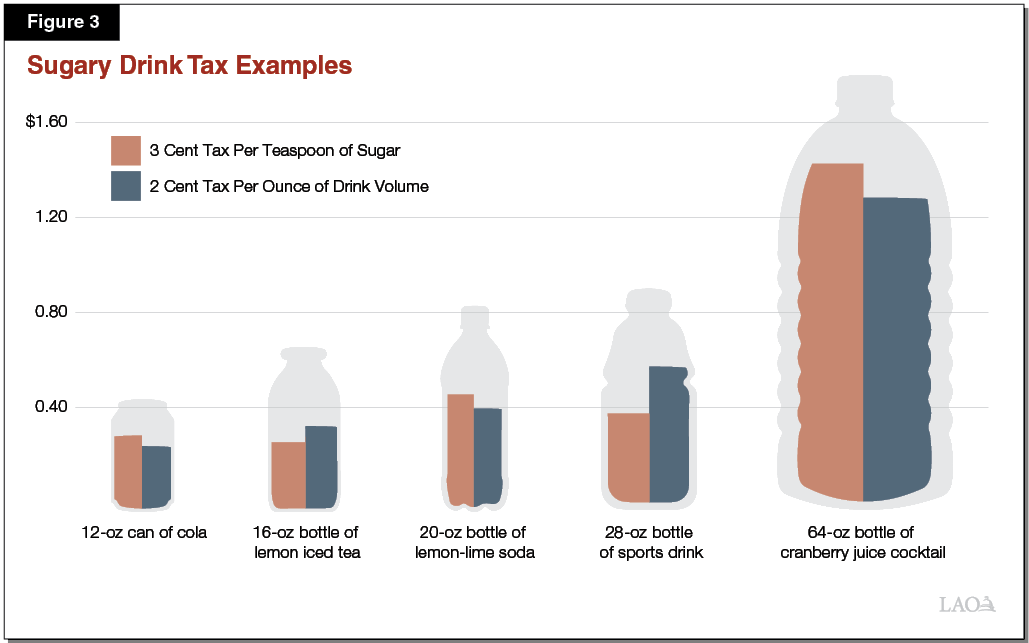
In the United States, the FDA regulates labeling but lacks direct authority over pricing structures, which are managed at municipal or state levels. Contrast this with the United Kingdom, where the Soft Drinks Industry Levy directly reformulated products by taxing sugar content rather than sales volume. The NYU study highlights a crucial divergence: US taxes target the transaction, whereas international models often target the formulation.
This distinction impacts patient access to healthier options. In jurisdictions with formulation taxes, manufacturers reduce sugar content to avoid levies, effectively lowering the glycemic load of the entire population’s diet. In the US fast-food model analyzed here, the product remains high-sugar and the consumer pays more without health benefit. This creates a regressive health outcome, where lower-income populations bear the financial cost without the metabolic protection.
“Fiscal policies are powerful tools, but they must be designed to encourage reformulation, not just revenue generation. If the sugar content remains unchanged, the public health victory is incomplete.”
— Dr. Tedros Adhanom Ghebreyesus, Director-General, World Health Organization (General Statement on Fiscal Policies for Health)
Funding Transparency and Data Integrity
Transparency in research funding is vital for establishing trust in medical journalism. This specific line of inquiry by Dr. Elbel and colleagues was supported by grants from the Robert Wood Johnson Foundation and the National Institutes of Health (NIH). These are non-profit and government entities, reducing the risk of industry bias that might otherwise minimize the harms of sugar consumption. However, readers must note that observational data cannot prove causation definitively; it establishes correlation within specific geographic boundaries.
To understand the broader context, we must appear at peer-reviewed meta-analyses regarding sugar intake and metabolic syndrome. The following table summarizes the comparative efficacy of different tax structures on health outcomes.
| Tax Model | Target | Impact on Purchases | Metabolic Benefit |
|---|---|---|---|
| US Sales Tax (Fast Food) | Transaction Price | Low/None | Minimal |
| UK Levy | Sugar Content | Moderate | High (Reformulation) |
| Mexico Excise Tax | Volume (Liter) | High | Moderate |
Clinical Implications for Patient Care
For practicing clinicians, this data reinforces the need for direct patient counseling over reliance on environmental changes. We cannot wait for policy to heal our patients. The pathophysiology of excess sugar intake involves hepatic lipogenesis, where the liver converts fructose into fat, contributing to non-alcoholic fatty liver disease (NAFLD). Whether the drink is taxed or not, this biological pathway remains active.
the study underscores the importance of social determinants of health. Fast-food deserts often lack grocery stores where taxes might be more effective. Patients in these areas face a dual burden: limited access to whole foods and exposure to high-calorie beverages that fiscal policy fails to mitigate. Healthcare providers must document dietary habits with the same rigor as medication adherence.
Contraindications & When to Consult a Doctor
While this article discusses policy, the clinical implications relate to dietary intake. Patients with insulin resistance, type 2 diabetes, or metabolic syndrome should treat sugary beverages as a contraindicated substance, regardless of price. There is no safe threshold for added sugar in these populations.
- Consult a Physician If: You experience polyuria (excessive urination), polydipsia (excessive thirst), or unexplained fatigue after consuming high-carbohydrate beverages.
- Avoid Reliance on Policy: Do not assume a “taxed” drink is safer. The sugar content remains the primary risk factor.
- Medication Interaction: High sugar intake can interfere with glycemic control medications, requiring dosage adjustments under medical supervision.
the trajectory of public health requires a multi-modal approach. Fiscal measures are merely one instrument in a larger orchestra that must include education, access to care, and industry reformulation. As we move forward in 2026, the focus must shift from punishing the consumer to engineering healthier defaults within the food supply chain.
References
- PLOS Medicine – Open Access Journal Publishing the Primary Study.
- Centers for Disease Control and Prevention (CDC) – Data on Sugar-Sweetened Beverage Intake.
- World Health Organization (WHO) – Guidelines on Sugar Intake for Adults and Children.
- PubMed Central – Archive of Biomedical and Life Sciences Journal Literature.
- National Institute of Diabetes and Digestive and Kidney Diseases – Diabetes Diet and Eating Guidelines.