
Tuberculosis (TB), a bacterial infection primarily affecting the lungs, is experiencing a global resurgence after decades of decline. Driven by factors including pandemic-related healthcare disruptions, underfunding of public health initiatives, and emerging drug resistance, cases are rising in both developed and developing nations, posing a renewed threat to global health security.
For centuries, Mycobacterium tuberculosis has been a formidable foe, responsible for over one billion deaths – exceeding the combined toll of smallpox, malaria, HIV/AIDS, cholera, and influenza. While the advent of antibiotics in the mid-20th century dramatically reduced TB incidence, complacency and dwindling resources have allowed the bacterium to regain a foothold. The current upswing isn’t merely a statistical blip; it signals systemic vulnerabilities in our approach to infectious disease control.
In Plain English: The Clinical Takeaway
- TB is contagious: It spreads through the air when someone with active TB coughs or sneezes.
- Not everyone gets sick: You can be infected with TB bacteria but not develop the disease (latent TB). However, latent TB can become active.
- Treatment is available: TB is curable with a course of antibiotics, but it’s crucial to complete the full treatment regimen to prevent drug resistance.
The Complexities of a Resurgent Threat
The recent increase in TB cases isn’t uniform. The United States, while maintaining relatively low overall incidence rates, witnessed a 7.9% increase in cases in 2024, according to the Centers for Disease Control and Prevention (CDC). This trend mirrors a similar pattern in the United Kingdom, where 2024 saw the largest single-year spike in TB cases since surveillance began in the 1990s. However, the most significant burden remains in low- and middle-income countries, particularly in Africa and Southeast Asia. The World Health Organization (WHO) reported a global rise in TB cases in 2024, reaching the highest level on record. This increase is particularly concerning in regions with high rates of HIV co-infection, as individuals with compromised immune systems are significantly more susceptible to developing active TB.
The mechanism of action of Mycobacterium tuberculosis is remarkably sophisticated. The bacterium possesses a unique cell wall rich in mycolic acids, rendering it resistant to many common antibiotics and hindering the host’s immune response. Upon inhalation, the bacteria are engulfed by macrophages – immune cells designed to destroy pathogens. However, M. Tuberculosis can survive and even replicate within these macrophages, effectively hiding from the immune system. This intracellular survival is facilitated by the bacterium’s ability to inhibit phagosome-lysosome fusion, a critical step in the macrophage’s killing process. The development of active TB disease depends on a complex interplay between bacterial factors, host immune responses, and environmental factors.
The Impact of Funding Cuts and Political Shifts
The resurgence of TB is inextricably linked to political and economic factors. The reduction in federal funding for TB programs in the US, beginning in 1972, created a critical vulnerability. More recently, funding cuts to global health initiatives by the Trump Administration, as highlighted by analyses from Harvard and Boston Universities, are projected to lead to a staggering increase in TB cases and deaths, particularly among children. These cuts threaten to reverse decades of progress in TB control, especially in countries heavily reliant on external aid. Leonardo Martinez, assistant professor of epidemiology at Boston University School of Public Health, stated in a press release, “The heaviest toll would fall on low-income countries in Africa and Southeast Asia, and in settings where HIV and TB overlap and health systems rely heavily on external aid.”
The Global Fund to Fight AIDS, Tuberculosis and Malaria, a key international funding mechanism, has been instrumental in reducing TB incidence globally. However, sustained funding is crucial to maintain this momentum. A potential withdrawal of US support from the Global Fund would have catastrophic consequences, potentially leading to nearly 9 million childhood TB cases and over 1.5 million child deaths over the next decade. This underscores the interconnectedness of global health security and the importance of sustained international cooperation.
Drug Resistance and the Pipeline for Latest Treatments
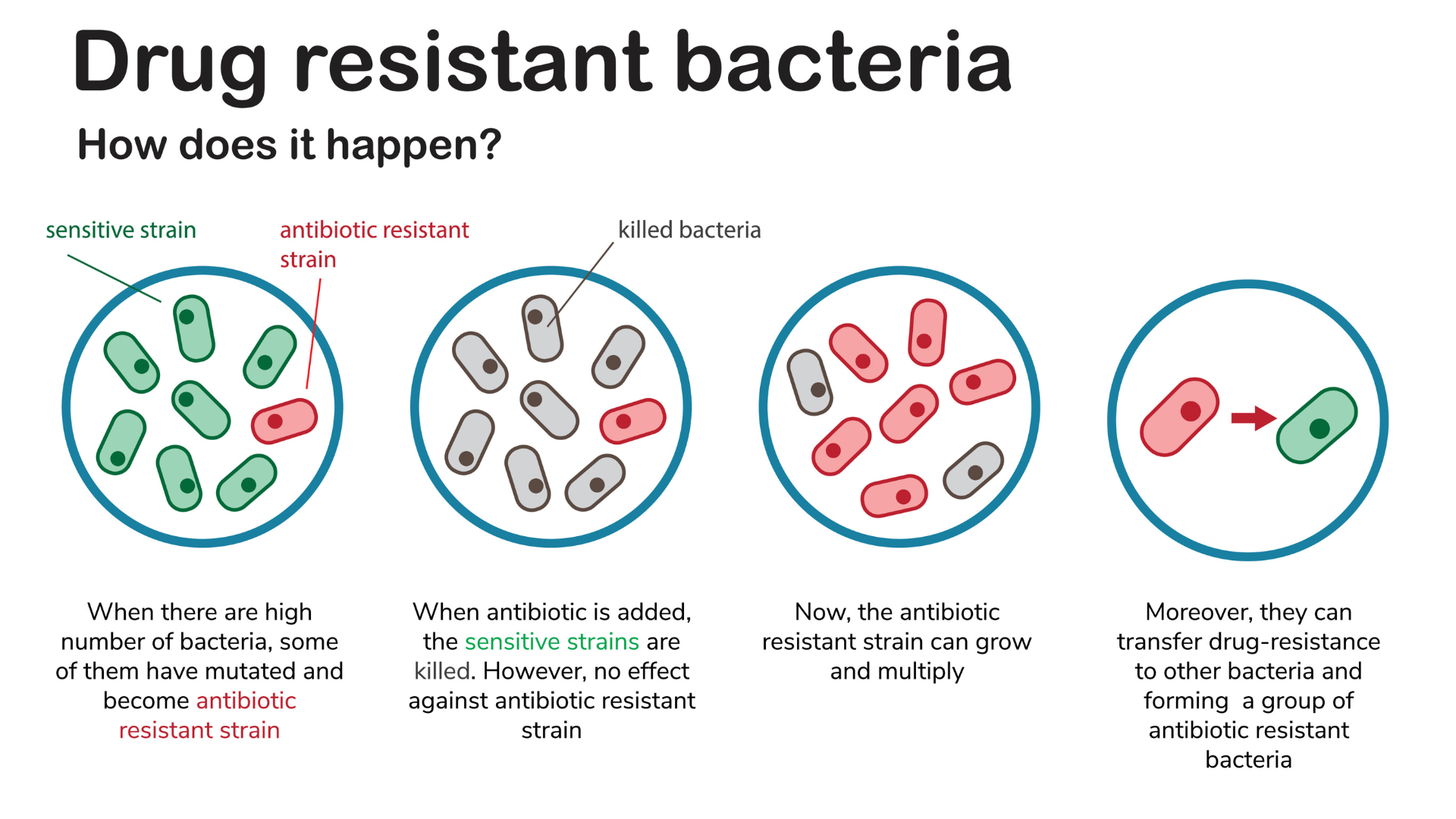
A particularly alarming aspect of the TB resurgence is the increasing prevalence of drug-resistant strains, including multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB). MDR-TB is defined as resistance to at least isoniazid and rifampicin, the two most potent first-line anti-TB drugs. XDR-TB exhibits resistance to isoniazid, rifampicin, and at least one of the fluoroquinolones or a second-line injectable drug. Treatment of drug-resistant TB requires prolonged courses of second-line drugs, which are often more toxic and less effective.
The development of new anti-TB drugs is a critical priority. Bedaquiline, approved by the FDA in 2012, was the first new anti-TB drug in nearly 40 years. Delamanid, approved by the European Medicines Agency (EMA) in 2014, represents another important addition to the treatment arsenal. However, these drugs are expensive and not widely available in many high-burden countries. Pretomanid, a nitroimidazole drug, has shown promising results in combination with bedaquiline and linezolid for the treatment of MDR-TB. Clinical trials have demonstrated high rates of treatment success with this regimen, offering hope for patients with drug-resistant disease. The ongoing Phase III trials of novel compounds targeting different mechanisms of action are crucial for expanding the treatment options and combating drug resistance.
| Drug | Mechanism of Action | Typical Side Effects | Efficacy (MDR-TB) |
|---|---|---|---|
| Bedaquiline | Inhibits mycobacterial ATP synthase | QT prolongation, nausea, vomiting | ~79% treatment success |
| Delamanid | Inhibits mycolic acid synthesis | QT prolongation, nausea, vomiting | ~68% treatment success |
| Pretomanid (with Bedaquiline & Linezolid) | Nitroimidazole; disrupts bacterial energy metabolism | Peripheral neuropathy, myelosuppression | ~90% treatment success |
Contraindications & When to Consult a Doctor
Individuals with known allergies to any of the anti-TB medications should inform their healthcare provider. Patients with pre-existing liver disease or kidney problems require careful monitoring during treatment. Pregnant or breastfeeding women should discuss the risks and benefits of anti-TB therapy with their doctor. Anyone experiencing symptoms suggestive of TB – a persistent cough lasting more than three weeks, chest pain, fever, night sweats, weight loss, or fatigue – should seek medical attention immediately. Early diagnosis and treatment are crucial for preventing the spread of infection and improving patient outcomes.
The resurgence of tuberculosis is a stark reminder that infectious diseases remain a significant threat to global health. Addressing this challenge requires a multifaceted approach, including increased funding for research and public health programs, improved access to diagnosis and treatment, and a renewed commitment to international cooperation. As Dr. Mario Raviglione, former Director of the WHO’s Global Tuberculosis Programme, emphasized, “TB is a disease of poverty and inequality. Addressing the social determinants of health is essential for achieving TB elimination.” The fight against TB is far from over, and sustained vigilance is paramount.
References
- World Health Organization. (2025). Global Tuberculosis Report 2025.
- Centers for Disease Control and Prevention. (2024). Tuberculosis Surveillance Report, 2024.
- Martinez, L., et al. (2025). Potential impact of US funding cuts on global tuberculosis burden. The Lancet Global Health.
- Raviglione, M. C. (2019). Tuberculosis 2019. The New England Journal of Medicine, 380(22), 2149-2158.
- Korenromp, E. L., et al. (2021). The impact of COVID-19 on tuberculosis diagnosis and treatment. International Journal of Tuberculosis and Lung Disease, 25(1), 3-11.