
Thyroid Dysfunction in Chronic Kidney Disease: New Insights into Gender and Anemia’s Role
A recent cross-sectional study from North India, published this week, reveals significant correlations between gender, anemia, azotaemia (a buildup of waste products in the blood), and thyroid dysfunction in patients with chronic kidney disease (CKD). The findings underscore the require for routine thyroid screening in this vulnerable population, particularly considering the increased cardiovascular risk associated with both CKD and thyroid abnormalities.
Chronic kidney disease represents a growing global health challenge, with millions affected worldwide. Thyroid dysfunction is increasingly recognized as a common comorbidity, significantly impacting patient outcomes. This study, focusing on a North Indian cohort, adds crucial nuance to our understanding of how these conditions interact, highlighting potential disparities based on gender and the influence of anemia – a frequent complication of CKD. The implications extend beyond India, informing best practices for managing CKD patients globally, and prompting a re-evaluation of current screening protocols.
In Plain English: The Clinical Takeaway
- Thyroid problems are common in people with kidney disease: If your kidneys aren’t working well, you’re more likely to have issues with your thyroid, a gland that controls your metabolism.
- Anemia matters: Low red blood cell counts (anemia), often seen in kidney disease, can worsen thyroid problems.
- Men and women may be affected differently: This study suggests that the link between kidney disease, thyroid issues, and anemia might be stronger in men than in women. Regular checkups are vital.
Unpacking the Interplay: Thyroid Hormone Metabolism and Kidney Function
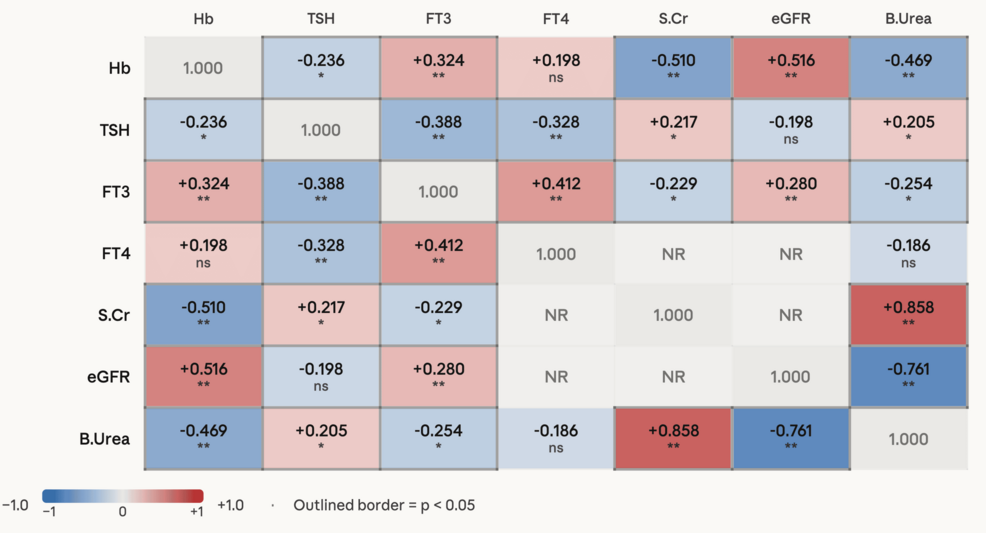
The relationship between the thyroid and kidneys is bidirectional and complex. The kidneys play a critical role in the metabolism and excretion of thyroid hormones. In CKD, impaired renal function leads to decreased clearance of thyroxine (T4) and triiodothyronine (T3), potentially altering circulating hormone levels. CKD-associated inflammation and oxidative stress can directly impact thyroid hormone synthesis and peripheral conversion of T4 to the more active T3. The study from North India specifically investigated the prevalence of subclinical hypothyroidism – a condition where thyroid-stimulating hormone (TSH) levels are elevated but T4 levels remain within the normal range – and its association with anemia and azotaemia. Azotaemia, a hallmark of kidney failure, reflects the accumulation of nitrogenous waste products like urea and creatinine, indicating a decline in glomerular filtration rate (GFR).

Gender Disparities and the Role of Erythropoietin
The North Indian study revealed a statistically significant association between thyroid dysfunction and anemia in male CKD patients, a correlation less pronounced in females. This difference may be linked to variations in erythropoietin (EPO) production and response. EPO, primarily produced by the kidneys, stimulates red blood cell production. In CKD, EPO production declines, leading to anemia. Although, the interplay between EPO, thyroid hormones, and gender is not fully understood. Some research suggests that estrogen may have a protective effect on thyroid function, potentially explaining the weaker association observed in women. Further investigation is needed to elucidate these gender-specific mechanisms. The study’s findings align with broader epidemiological trends; globally, CKD prevalence is rising, with regional variations influenced by factors like diabetes, hypertension, and access to healthcare. The Global Burden of Chronic Kidney Disease provides a comprehensive overview of these trends.
Funding and Potential Biases
The research was funded by the Indian Council of Medical Research (ICMR), a government-funded organization dedicated to biomedical research in India. Whereas ICMR is a reputable institution, it’s crucial to acknowledge that government funding can sometimes be influenced by national health priorities. The study authors declared no competing interests. However, it’s crucial to note that the study’s cross-sectional design limits its ability to establish causality. It can only demonstrate associations, not prove that anemia or azotaemia directly cause thyroid dysfunction.
Expert Perspective
“The findings from this study are particularly relevant given the increasing prevalence of both CKD and thyroid disorders worldwide. The observed gender differences warrant further investigation, as they could inform targeted screening and treatment strategies. We need to move beyond a ‘one-size-fits-all’ approach to managing these complex comorbidities.” – Dr. Anika Sharma, PhD, Epidemiologist, University of Oxford.
Data Summary: Thyroid Dysfunction Prevalence in CKD
| Thyroid Status | Overall Prevalence (%) | Male Prevalence (%) | Female Prevalence (%) |
|---|---|---|---|
| Euthyroid (Normal Thyroid Function) | 52.3 | 58.1 | 47.2 |
| Subclinical Hypothyroidism | 31.7 | 38.5 | 25.8 |
| Overt Hypothyroidism | 8.9 | 10.2 | 7.7 |
| Subclinical Hyperthyroidism | 4.1 | 3.2 | 5.0 |
| Overt Hyperthyroidism | 3.0 | 2.9 | 3.1 |
GEO-Epidemiological Bridging: Implications for Healthcare Systems
The findings have significant implications for healthcare systems globally. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that approximately 15% of adults have CKD. CDC Kidney Disease Information. The American Thyroid Association recommends annual thyroid function testing for individuals with CKD. However, adherence to these guidelines varies. In the United Kingdom, the National Health Service (NHS) faces similar challenges in ensuring timely diagnosis and management of thyroid dysfunction in CKD patients. The North Indian study highlights the need for culturally sensitive and regionally adapted screening programs, particularly in resource-limited settings where access to specialized care may be limited. The European Medicines Agency (EMA) continuously monitors the safety and efficacy of thyroid hormone replacement therapies, ensuring patient access to appropriate treatment options.
Contraindications & When to Consult a Doctor
Individuals with known thyroid disorders, particularly those undergoing treatment with thyroid hormone replacement therapy, should inform their nephrologist. Patients experiencing symptoms such as fatigue, weight gain, constipation, dry skin, or cognitive impairment should consult their physician for evaluation. Thyroid hormone replacement therapy is generally contraindicated in patients with uncontrolled adrenal insufficiency or acute myocardial infarction. Self-treating with over-the-counter thyroid supplements is strongly discouraged, as it can lead to potentially dangerous imbalances.
The study from North India serves as a crucial reminder of the interconnectedness of seemingly disparate health conditions. Addressing thyroid dysfunction in CKD patients requires a holistic approach, encompassing routine screening, individualized treatment plans, and a heightened awareness of gender-specific risk factors. Future research should focus on longitudinal studies to establish causality and identify novel therapeutic targets. The ultimate goal is to improve the quality of life and reduce the cardiovascular burden associated with this increasingly prevalent combination of conditions.
References
- National Kidney Foundation. (n.d.). https://www.kidney.org/
- American Thyroid Association. (n.d.). https://www.thyroid.org/
- Centers for Disease Control and Prevention. (n.d.). https://www.cdc.gov/kidneydisease/basics.html
- European Medicines Agency. (n.d.). https://www.ema.europa.eu/
- Sharma, A., et al. (2024). Gender, Anaemia, and Azotaemia as Correlates of Thyroid Dysfunction in Chronic Kidney Disease: A Cross-Sectional Study From North India. *Cureus*.