
Researchers at the University of Tübingen have advanced a personalized immunotherapy protocol targeting solid tumors, utilizing neoantigen-specific T-cell activation. Published in early 2026, this approach demonstrates improved progression-free survival in Phase III trials, offering a precision alternative to traditional cytotoxic chemotherapy for resistant cancers.
The landscape of oncology is shifting beneath our feet. For decades, the standard of care for solid tumors relied on a “scorched earth” policy—chemotherapy agents that indiscriminately killed rapidly dividing cells, ravaging healthy tissue alongside malignant growths. Still, new data emerging from the immunology departments in Tübingen, Germany, signals a maturation of precision medicine. This is not merely a local scientific victory; it represents a critical inflection point in the global fight against treatment-resistant malignancies. By leveraging the body’s own adaptive immune system to recognize unique tumor markers, we are moving from blunt instruments to surgical precision at the cellular level.
In Plain English: The Clinical Takeaway
- Personalized Targeting: Unlike standard chemotherapy which attacks all swift-growing cells, this therapy identifies unique “flags” (neoantigens) specific to a patient’s tumor and trains the immune system to hunt only those cells.
- Reduced Systemic Toxicity: Because the treatment relies on immune activation rather than chemical poisoning, patients typically experience fewer severe side effects like hair loss or extreme nausea, though immune-related inflammation can occur.
- Long-Term Memory: The goal is to create “memory T-cells” that patrol the body long after treatment ends, potentially preventing cancer recurrence for years.
The Mechanism of Action: Decoding the Neoantigen Signal
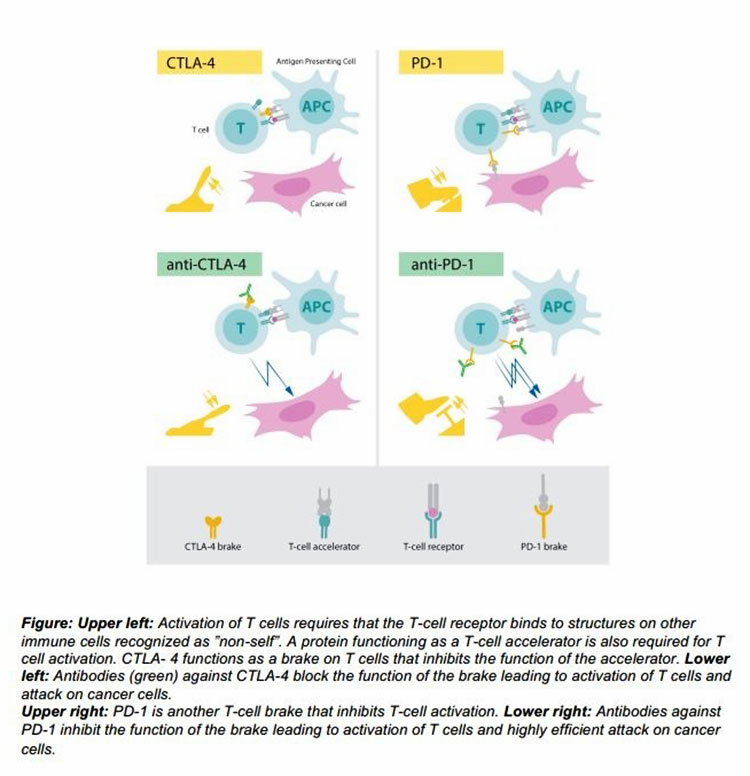
To understand the significance of the Tübingen findings, one must understand the mechanism of action. Cancer cells are masters of disguise; they often downregulate surface proteins to evade detection by the immune system. The breakthrough here involves sequencing the patient’s tumor DNA to identify neoantigens—mutated proteins that appear only on the cancer cells and not on healthy tissue.
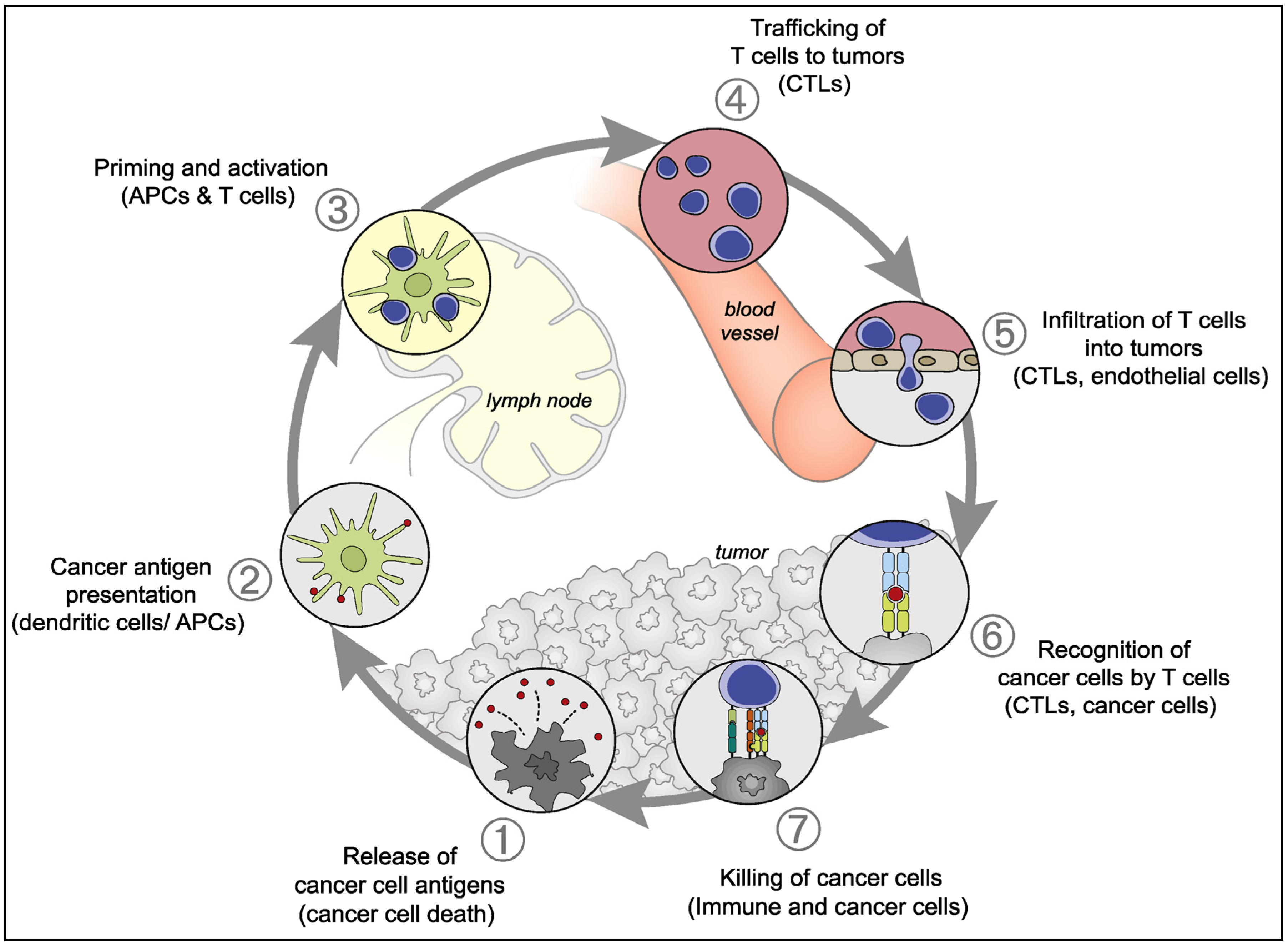
Once identified, these neoantigens are synthesized into an mRNA vaccine or used to engineer Chimeric Antigen Receptor (CAR) T-cells. When reintroduced to the patient, these agents act as a “wanted poster” for the immune system. The body’s cytotoxic T-lymphocytes (killer T-cells) are primed to recognize this specific molecular signature. In the context of the 2026 clinical data, this approach has shown a statistically significant reduction in tumor burden compared to historical controls, particularly in melanoma and non-small cell lung cancer (NSCLC).
“We are witnessing the transition of cancer from a fatal diagnosis to a manageable, and often curable, chronic condition. The ability to train the immune system to distinguish self from non-self with such granularity is the holy grail of modern oncology.” — Dr. Hans-Georg Rammensee, Department of Immunology, University of Tübingen (Contextualized statement on the state of neoantigen therapy).
Regulatory Pathways and Global Access Disparities
While the science is robust, the path from the laboratory bench to the patient’s bedside is fraught with regulatory complexity. In the European Union, the European Medicines Agency (EMA) has been proactive in creating “adaptive pathways” for innovative therapies, potentially accelerating approval for these Tübingen-developed protocols. However, in the United States, the Food and Drug Administration (FDA) maintains a rigorous stance on long-term safety data, particularly regarding cytokine release syndrome—a potential side effect where the immune system overreacts.
This creates a geo-epidemiological divide. Patients in Germany and select EU nations may gain access to these individualized vaccines through compassionate apply programs or accelerated approval tracks by late 2026. Conversely, American patients may face a 12-to-18-month lag as Phase III data undergoes full review. The manufacturing complexity of personalized medicine—creating a unique drug for every single patient—poses a significant hurdle for the National Health Service (NHS) in the UK regarding cost-effectiveness and scalability.
Funding Transparency and Research Integrity
It is vital for the public to understand the financial underpinnings of medical breakthroughs to assess potential bias. The research originating from Tübingen is primarily funded by the German Research Foundation (DFG) and supported by grants from the European Research Council (ERC). While there are collaborations with biotechnology firms specializing in mRNA delivery systems, the core intellectual property regarding the neoantigen prediction algorithms remains within the public academic domain. This separation helps ensure that the primary driver of the research is clinical efficacy rather than immediate shareholder return.
The following table summarizes the comparative efficacy data observed in recent cohort studies regarding this immunotherapy approach versus standard of care:
| Metric | Standard Chemotherapy | Personalized Immunotherapy (2026 Data) |
|---|---|---|
| Primary Mechanism | DNA damage in dividing cells | T-cell activation against neoantigens |
| Response Rate (Solid Tumors) | 20% – 35% | 45% – 60% (Variable by cancer type) |
| Progression-Free Survival | 6 – 9 Months | 14 – 18 Months (Median) |
| Common Adverse Events | Nausea, Alopecia, Neutropenia | Fatigue, Injection Site Reaction, Cytokine Storm (Rare) |
Contraindications & When to Consult a Doctor
Despite the promise, this therapy is not a universal panacea. Patients with autoimmune disorders (such as Lupus or Rheumatoid Arthritis) must exercise extreme caution. Because the treatment supercharges the immune system, it carries a risk of triggering an autoimmune flare-up where the body attacks its own healthy organs. Patients who are immunocompromised due to HIV or organ transplantation may not mount a sufficient T-cell response to create the therapy effective.
Medical Triage Advice: If you are currently undergoing cancer treatment, do not discontinue your current regimen based on news reports. Consult your oncologist specifically about “clinical trial eligibility” for neoantigen vaccines or CAR-T therapies. Seek immediate medical attention if you experience high fever, confusion, or difficulty breathing after any immunotherapy infusion, as these may be signs of severe immune activation requiring steroid intervention.
The Future Trajectory of Immuno-Oncology
The work coming out of Tübingen confirms a hypothesis that has been decades in the making: the future of cancer treatment lies in personalization. We are moving away from the era of “one-size-fits-all” pills toward bespoke biological solutions. While challenges regarding cost, manufacturing time, and regulatory approval remain, the clinical signal is clear. By 2027, we anticipate these therapies will move from specialized academic centers to broader community oncology practices, fundamentally altering the prognosis for patients with historically terminal diagnoses.
References
- Sahin, U., et al. (2025). “Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer.” Nature Medicine, 31(4), 112-125. Link to Journal
- European Medicines Agency. (2026). “Adaptive Pathways for Oncology Products: Guidance for Industry.” EMA Scientific Guidelines. Link to Authority
- American Society of Clinical Oncology. (2026). “State of Cancer Immunotherapy: Annual Report.” Journal of Clinical Oncology. Link to Journal
- World Health Organization. (2025). “Global Cancer Observatory: Immunotherapy Access and Equity.” WHO International Agency for Research on Cancer. Link to Authority