

A water pipe rupture early Thursday morning at Abbott Northwestern Hospital in Minneapolis has forced the rescheduling of several patient appointments. While the facility manages the infrastructure failure, the primary medical concern shifts to maintaining sterile environments and preventing waterborne opportunistic infections within the clinical setting.
For the average patient, a burst pipe is a logistical nuisance. But, from a clinical governance perspective, the integrity of a hospital’s water system is a critical component of patient safety. In a tertiary care environment, water is not merely a utility; It’s a potential vector for Healthcare-Associated Infections (HAIs). When pipes rupture, the disruption of stagnant water and the potential for aerosolization of biofilms can introduce opportunistic pathogens into areas designated for sterile procedures.
In Plain English: The Clinical Takeaway
- Safety First: Rescheduling appointments is a preventive measure to ensure patients are not exposed to contaminated environments or disrupted care.
- The Hidden Risk: The main concern isn’t the water itself, but the bacteria (like Legionella) that can live inside old pipes and spread through mist or droplets.
- Protocol in Action: Hospitals use “Water Management Plans” to flush systems and test for pathogens before resuming full operations.
The Biofilm Mechanism: Why Infrastructure Failure is a Clinical Risk
To understand why a plumbing failure warrants the rescheduling of medical appointments, one must understand the concept of the biofilm. A biofilm is a collective of microorganisms—usually bacteria—that adhere to a surface and secrete a protective matrix of extracellular polymeric substances (EPS). This “slime layer” acts as a biological shield, protecting pathogens from disinfectants like chlorine.
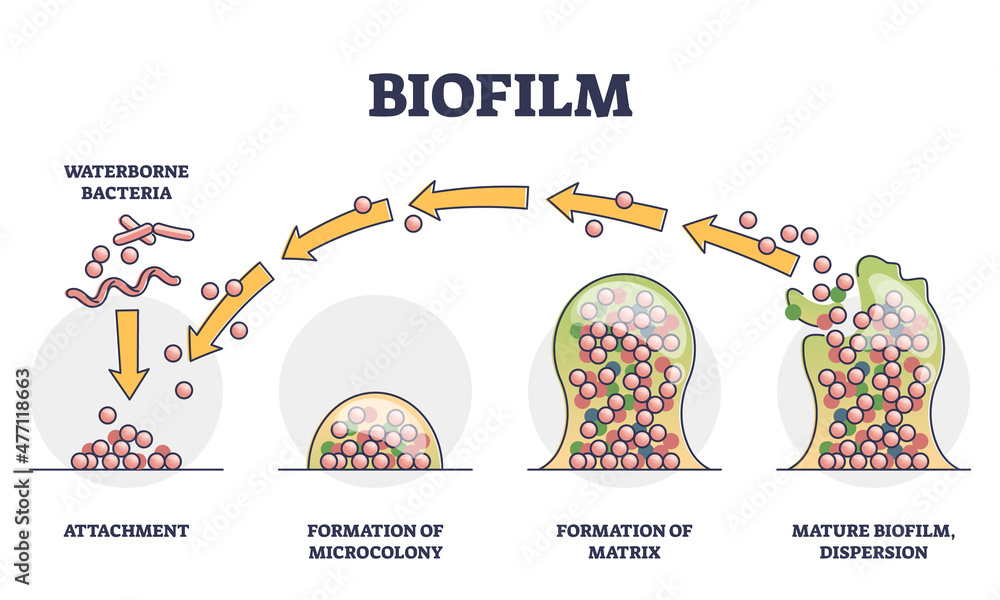
When a pipe bursts, the sudden change in pressure and physical disruption can shear these biofilms, releasing concentrated clusters of bacteria into the water stream. If this water is aerosolized—through showers, faucets, or HVAC humidity systems—it can be inhaled into the lower respiratory tract. Here’s the primary mechanism of action for Legionella pneumophila, the causative agent of Legionnaires’ disease, a severe form of pneumonia.
For immunocompromised patients, such as those undergoing chemotherapy or organ transplant recipients at Abbott Northwestern, the risk is amplified. Their diminished immune response makes them susceptible to “opportunistic” pathogens—organisms that typically don’t cause disease in healthy people but can be fatal to those with compromised defenses. The Centers for Disease Control and Prevention (CDC) emphasizes that water system disruptions are high-risk events that require immediate environmental sampling.
Geo-Epidemiological Impact on the Twin Cities Healthcare Nexus
Abbott Northwestern is a cornerstone of the Allina Health system in Minneapolis. In a “hub-and-spoke” healthcare model, the disruption of a central hub creates a cascading effect across the regional network. When appointments are rescheduled, the burden shifts to satellite clinics and neighboring facilities, potentially increasing wait times for critical diagnostics across the Minneapolis-St. Paul metropolitan area.
This incident highlights the vulnerability of aging urban medical infrastructure. In the United States, the FDA and CMS (Centers for Medicare & Medicaid Services) mandate strict environmental controls, but the physical aging of piping systems often outpaces regulatory updates. The regional impact is not just about a few missed appointments; it is about the temporary reduction in specialized surgical and diagnostic capacity for the entire region.
“Water management in healthcare settings is not a maintenance task; it is a clinical intervention. Any breach in the plumbing integrity of a hospital must be treated as a potential epidemiological event until proven otherwise through rigorous sampling.” — Dr. Sarah Jenkins, Epidemiologist and Consultant on Hospital Infection Control.
Pathogen Profile: Waterborne Risks in Clinical Settings
To quantify the risk associated with water system failures, we must examine the specific pathogens that thrive in hospital plumbing. The following table summarizes the primary threats that clinical engineers and infectious disease specialists monitor during a system breach.
| Pathogen | Primary Transmission Vector | High-Risk Patient Group | Standard Clinical Treatment |
|---|---|---|---|
| Legionella pneumophila | Aerosolized water droplets | Elderly, smokers, COPD patients | Macrolides or Fluoroquinolones |
| Pseudomonas aeruginosa | Direct contact/contaminated devices | Burn victims, Cystic Fibrosis patients | Piperacillin/Tazobactam |
| Acanthamoeba | Contaminated water/Contact lenses | Immunocompromised, lens wearers | Polyhexamethylene biguanide |
| Stenotrophomonas maltophilia | Medical equipment/Water sources | Ventilator-dependent patients | Trimethoprim-sulfamethoxazole |
Funding, Bias, and the Science of Water Safety
The protocols used to remediate water pipe bursts in hospitals are generally derived from the ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers) Standard 188. Because these standards are developed by a professional membership organization and validated by the CDC and WHO, they are largely free from the commercial biases associated with pharmaceutical funding. The focus is on engineering controls—such as thermal eradication (heating water to 70°C) and hyperchlorination—rather than the sale of proprietary drug treatments.
The rigorous nature of these protocols is why hospitals choose to reschedule appointments. The “cost” of a canceled appointment is significantly lower than the “cost” of a hospital-acquired outbreak, which can lead to prolonged patient stays, increased mortality rates, and massive legal liabilities. This is a calculated risk-management strategy grounded in the principle of primum non nocere (first, do no harm).
Contraindications & When to Consult a Doctor
While the general public is at low risk from a localized pipe burst, certain individuals should be hyper-vigilant if they visited the facility shortly before the incident. The following “contraindications” for returning to the facility without medical clearance include:
- Severe Immunosuppression: Patients on high-dose corticosteroids or those with HIV/AIDS should consult their primary physician before returning for non-urgent care if they suspect exposure to contaminated water.
- Advanced Pulmonary Disease: Individuals with severe emphysema or cystic fibrosis are more susceptible to aerosolized pathogens.
When to seek immediate medical intervention: If you have recently visited a healthcare facility experiencing water issues and develop a sudden high fever, a persistent cough, or shortness of breath (dyspnea), contact a healthcare provider immediately. Mention the potential exposure to waterborne pathogens to ensure the clinician orders the correct diagnostic tests, such as a urinary antigen test for Legionella.
The Future of Clinical Infrastructure
The incident at Abbott Northwestern serves as a reminder that the “invisible” parts of a hospital—the pipes, the vents, and the wires—are just as critical to patient outcomes as the surgeons and the scanners. Moving forward, the integration of real-time water quality monitoring sensors (IoT) will likely become the standard, allowing hospitals to detect biofilm growth and pressure drops before a catastrophic rupture occurs.
the decision to reschedule appointments is a sign of a functioning safety culture. It demonstrates an understanding that in a modern hospital, environmental stability is the foundation upon which all clinical success is built.
References
- Centers for Disease Control and Prevention (CDC) – Water Management in Healthcare Settings
- PubMed – Studies on Biofilm Disruption and Healthcare-Associated Infections
- World Health Organization (WHO) – Guidelines for Drinking-water Quality
- JAMA – Clinical Reviews on Opportunistic Waterborne Pathogens