
When a pregnancy implants outside the uterus, typically in a fallopian tube, it is classified as an ectopic pregnancy. This condition is non-viable and poses significant health risks, including rupture and hemorrhage. Even as often associated with natural conception, assisted reproductive technologies (IVF) carry a nuanced risk profile requiring vigilant clinical monitoring and immediate medical intervention.
The recent public disclosure regarding pregnancy loss during an IVF journey highlights a critical, often silenced complication in reproductive medicine. For patients navigating fertility treatments, understanding the clinical reality of ectopic implantation is vital. This represents not merely an emotional loss but a specific medical event requiring precise management. As we analyze the intersection of celebrity disclosure and public health, the focus must remain on epidemiological data, treatment safety and the physiological mechanisms that dictate patient outcomes in 2026.
In Plain English: The Clinical Takeaway
- Viability: An ectopic pregnancy cannot develop into a live birth because the tissue outside the uterus cannot support the growing embryo.
- Risk Factor: IVF procedures slightly elevate the risk of ectopic implantation compared to natural conception due to embryo transfer dynamics.
- Urgency: Symptoms like sharp abdominal pain or bleeding require immediate emergency care to prevent life-threatening internal bleeding.
The Mechanism of Ectopic Implantation in ART
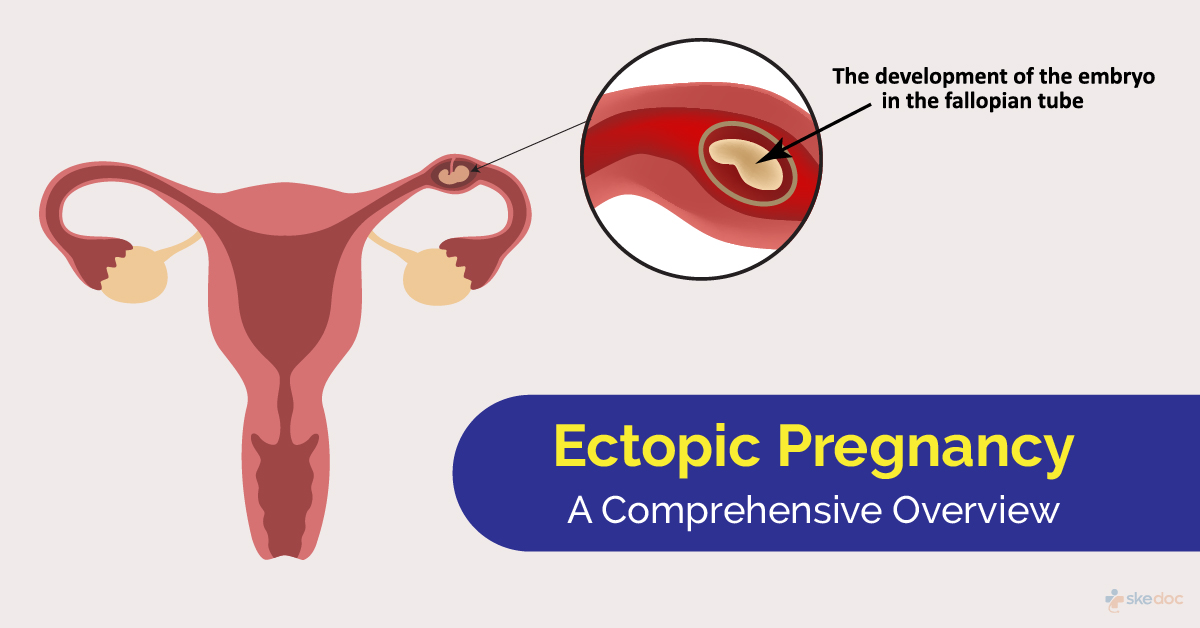
In a standard physiological process, the fertilized egg travels down the fallopian tube to implant in the uterine lining. In ectopic pregnancies, this migration is disrupted. The embryo implants in the fallopian tube, ovary, or abdominal cavity. Within the context of In Vitro Fertilization (IVF), the mechanism involves the direct placement of the embryo into the uterine cavity. Although, retrograde flow or uterine contractions can inadvertently push the embryo back into the tubal ostia.
Clinical terminology refers to this as tubal implantation. The trophoblast cells, which form the placenta, invade the tubal wall. Unlike the uterus, the fallopian tube lacks the decidual tissue necessary to accommodate this invasion. As the embryo grows, it stretches the tube, leading to pain and potential rupture. This mechanism of action explains why early detection via transvaginal ultrasound and serial beta-hCG monitoring is the gold standard for safety.
Epidemiological Realities and Risk Stratification
Public health data indicates that ectopic pregnancy occurs in approximately 1.5% to 2% of all reported pregnancies. Among patients undergoing Assisted Reproductive Technology (ART), historical data suggests rates may range slightly higher, between 2% and 5%, depending on tubal factor infertility history. Recent longitudinal studies emphasize that prior tubal surgery or pelvic inflammatory disease significantly increases this probability.
Geo-epidemiological bridging reveals disparities in care access. In the United Kingdom, the National Health Service (NHS) provides comprehensive coverage for ectopic pregnancy management under emergency care protocols. Conversely, in the United States, coverage varies by insurance provider, though the Affordable Care Act mandates coverage for essential health benefits including emergency services. The European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) both regulate the pharmaceutical interventions used, ensuring safety standards across regions.
“Early diagnosis is the single most essential factor in reducing morbidity associated with ectopic pregnancy. Clinicians must maintain a high index of suspicion in any patient of reproductive age presenting with abdominal pain.” — American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin.
Transparency in funding is crucial for patient trust. Most large-scale epidemiological data on IVF outcomes is funded by national health registries, such as the CDC’s National Assisted Reproductive Technology Surveillance System in the US, or independent academic grants rather than pharmaceutical companies. This reduces commercial bias in the reporting of complication rates.
Treatment Protocols and Regulatory Oversight
Management strategies depend on the patient’s hemodynamic stability and the size of the ectopic mass. The two primary interventions are medical management using methotrexate or surgical intervention via laparoscopy. Methotrexate acts as a folate antagonist, stopping rapidly dividing cells from growing. This is strictly contraindicated in patients with liver or kidney dysfunction.
Surgical options include salpingostomy (making an incision in the tube to remove the pregnancy) or salpingectomy (removing the tube entirely). The choice depends on the desire for future fertility and the condition of the contralateral tube. Regulatory bodies ensure that these protocols adhere to strict safety guidelines to minimize future infertility risks.
| Intervention Type | Mechanism of Action | Success Rate | Primary Risk |
|---|---|---|---|
| Methotrexate | Stops cell division | ~90% (selected cases) | Drug toxicity, rupture |
| Laparoscopic Surgery | Physical removal | ~95% | Anesthesia, scarring |
| Expectant Management | Natural resolution | ~70% (low hCG) | Unexpected rupture |
Contraindications & When to Consult a Doctor
Patients undergoing IVF must be aware of specific warning signs. Methotrexate treatment is contraindicated for individuals with immunodeficiency, active pulmonary disease, or breastfeeding. If a patient experiences sudden, severe abdominal pain, shoulder tip pain (referred pain from diaphragmatic irritation), or dizziness, this indicates potential rupture and hemorrhage.
Immediate consultation is required if beta-hCG levels do not decline appropriately after treatment. Persistent trophoblastic tissue can lead to continued bleeding. Patients should not rely on home pregnancy tests alone for monitoring resolution, as they remain positive until hCG clears the system completely. Professional serial blood testing is the only valid method for confirming treatment success.
The emotional toll of pregnancy loss, particularly amidst high-investment treatments like IVF, is profound. However, clinical safety must precede emotional processing. Understanding the statistical probability of ectopic events allows patients to engage with their care teams more effectively. By demystifying the clinical pathway, we empower patients to recognize risks early and seek the life-saving intervention they require.
References
- Centers for Disease Control and Prevention (CDC) – Infertility and ART
- American College of Obstetricians and Gynecologists (ACOG) – Ectopic Pregnancy
- American Society for Reproductive Medicine (ASRM) – Practice Guidelines
- National Library of Medicine (PubMed) – Ectopic Pregnancy Studies
- World Health Organization (WHO) – Maternal Health