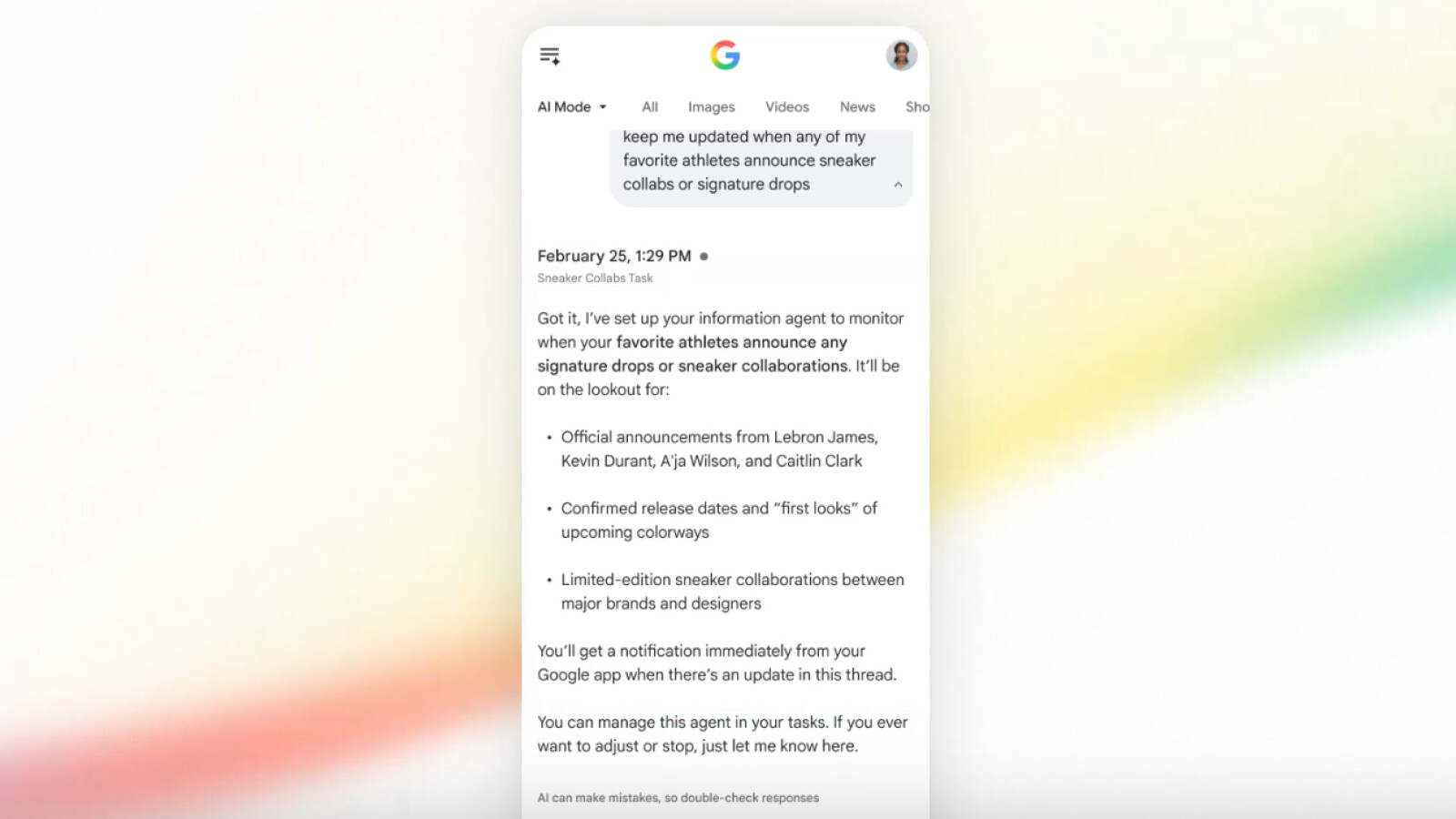
Google Launches Its Own OpenClaw Version
Google is rolling out its proprietary implementation of the OpenClaw framework this week, a strategic move designed to standardize high-performance tensor offloading across heterogeneous hardware environments. By decoupling AI inference ... Read More