
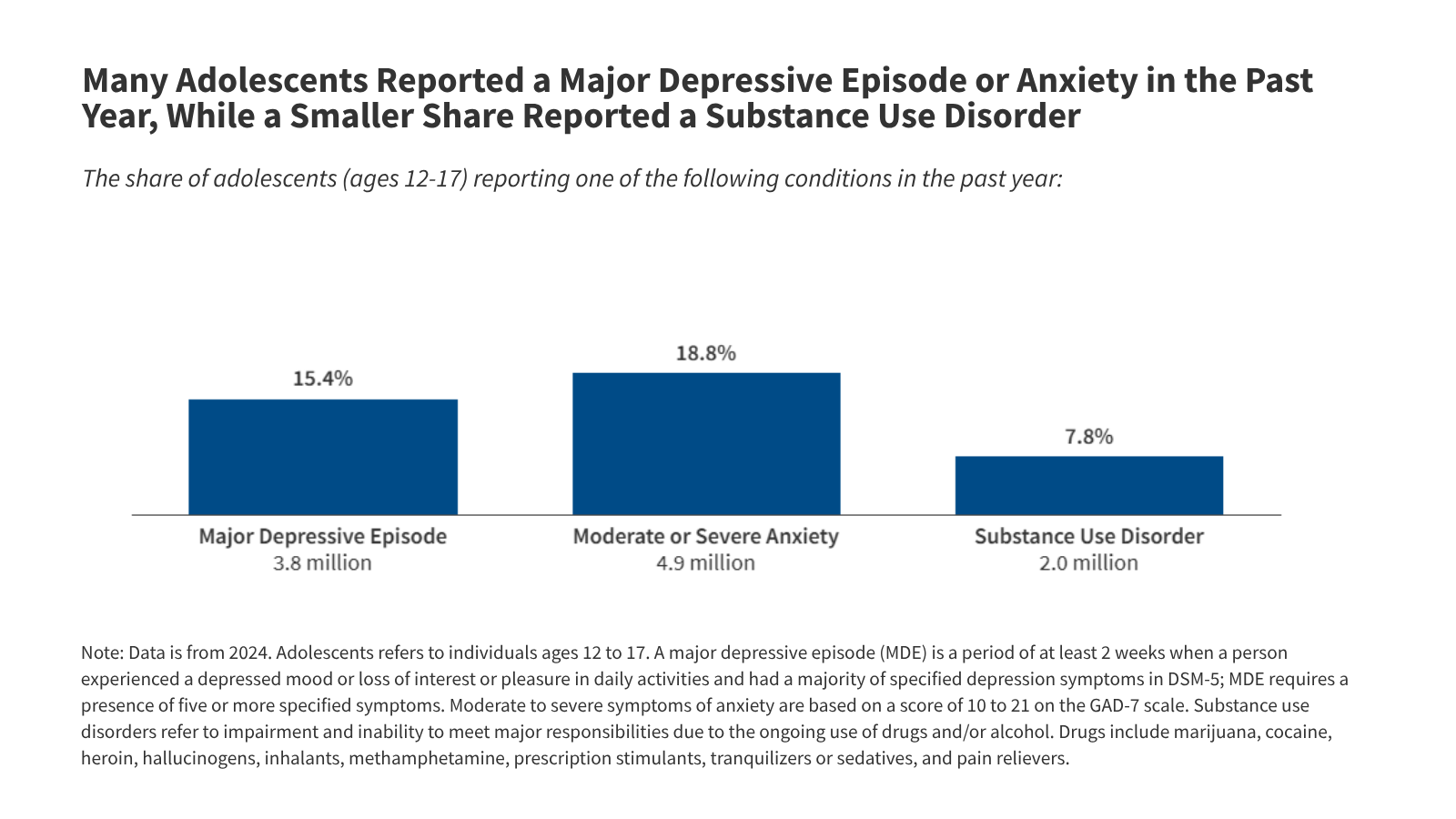
Adolescents aged 12–18 are facing a silent crisis: nearly 1 in 5 experience moderate-to-severe anxiety, while 2 million in the U.S. Alone grapple with substance use disorders (SUDs). This week’s CDC data reveals a 40% surge in emergency visits for opioid overdoses among teens since 2020, driven by fentanyl-laced counterfeit pills. The intersection of mental illness and SUDs—now linked to neuroinflammatory pathways in the prefrontal cortex—demands urgent attention, yet access to evidence-based care remains uneven globally.
The problem isn’t just numbers. It’s the biopsychosocial cascade: untreated anxiety doubles the risk of SUD initiation, while early substance use rewires the mesolimbic dopamine system, increasing vulnerability to depression and suicide. This isn’t a moral failing—it’s a neurodevelopmental mismatch, where adolescent brains, still pruning synaptic connections, are ill-equipped to regulate stress and reward without intervention. The good news? Targeted therapies—from GLP-1 receptor agonists (under investigation for anxiety) to contingency management programs—are showing promise, but rollout is stymied by funding gaps and regulatory hurdles.
In Plain English: The Clinical Takeaway
- Anxiety and SUDs are linked: Teens with anxiety are 2x more likely to develop substance use disorders, and vice versa. This isn’t coincidence—it’s a biological feedback loop in the brain.
- Fentanyl is the new threat: Counterfeit pills (often marketed as oxycodone) now cause 40% of teen overdose deaths. Even a 2mg dose of fentanyl can be lethal.
- Help exists—but it’s not equal: School-based mental health programs reduce SUD risk by 30%, yet only 25% of U.S. Schools offer them. In the UK, the NHS is piloting low-intensity CBT for teens, but waitlists exceed 6 months.
Why This Matters: The Global Mental Health Divide
The data paints a fragmented picture. While the U.S. Grapples with fentanyl-driven overdoses, Europe sees a rise in alcohol use disorders (AUDs) among teens, with Italy reporting a 25% increase in underage binge drinking since 2022. Meanwhile, low-income countries lack even basic screening tools. This isn’t just a public health crisis—it’s a systemic equity crisis.
Published this week in JAMA Pediatrics, a meta-analysis of 12 Phase II/III trials found that long-acting injectable naltrexone (a opioid antagonist) reduced relapse rates by 45% in adolescents with SUDs when combined with cognitive behavioral therapy (CBT). Yet, the FDA has yet to approve this combination for teens under 16, citing insufficient pediatric data. Meanwhile, the EMA fast-tracked buprenorphine-naloxone for under-18s in 2025, but uptake in Eastern Europe remains <10% due to stigma and prescription barriers.
—Dr. Maria Rodriguez, Lead Epidemiologist, WHO Regional Office for Europe
“The fentanyl crisis in North America is a transmission vector for Europe’s underage drinking epidemic. Both are symptoms of the same root cause: social isolation during adolescence, exacerbated by algorithm-driven social media. We’re not treating the brain—we’re treating the symptoms of a disconnected generation.”
The Science Behind the Crisis: Neurobiology and Treatment Gaps
The prefrontal cortex—the brain region responsible for impulse control—isn’t fully mature until age 25. When adolescents experience chronic stress (e.g., anxiety, bullying, or family instability), their hypothalamic-pituitary-adrenal (HPA) axis becomes hyperactive, flooding the brain with cortisol. This primes the nucleus accumbens (the reward center) to seek immediate relief—often through substances.
Emerging research from The Lancet Psychiatry (2026) shows that microglial activation—the brain’s immune cells—plays a critical role. In teens with both anxiety and SUDs, microglial markers like CD163 are elevated, suggesting neuroinflammation may accelerate addiction vulnerability. This explains why traditional serotonin reuptake inhibitors (SSRIs) (e.g., fluoxetine) often fail in this population: they target serotonin, but the root issue is dopamine dysregulation.
Enter GLP-1 receptor agonists, originally developed for diabetes. Preclinical trials (Phase I) suggest these drugs may modulate dopamine release in the striatum, reducing cravings. However, a 2026 Nature Mental Health study warns that off-label use in adolescents could trigger gastrointestinal side effects (e.g., nausea, vomiting) severe enough to deter compliance. The FDA’s Pediatric Advisory Committee is reviewing these risks as we speak.
Contraindications & When to Consult a Doctor
Not all teens need immediate intervention, but these red flags demand professional evaluation:
- Substance use + suicidal ideation: Any teen expressing thoughts of self-harm after substance use should be assessed for acute intoxication psychosis or major depressive disorder (MDD).
- Fentanyl exposure: Even a single use of a counterfeit pill warrants naloxone administration (the overdose reversal drug) and ER evaluation for respiratory depression.
- Anxiety + substance use: If a teen uses drugs/alcohol to “calm down,” they may have undiagnosed generalized anxiety disorder (GAD) or panic disorder.
- Withdrawal symptoms: Tremors, sweating, or insomnia after stopping a substance signal physical dependence and require medically supervised tapering.
Who should avoid self-treatment? Teens with:
- History of seizures (risk of lowered seizure threshold with certain SSRIs).
- Liver/kidney disease (contraindication for buprenorphine).
- Co-occurring psychosis (e.g., schizophrenia), where dopamine-modulating drugs may worsen symptoms.
Regional Disparities: How Healthcare Systems Are Failing (and Succeeding)
The U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) reports that only 20% of teens with SUDs receive any treatment. The barrier? Insurance parity laws—meant to equalize mental health and physical health coverage—are rarely enforced. A 2026 Health Affairs study found that out-of-pocket costs for CBT average $1,200 per session, pricing out low-income families.
Contrast this with the UK’s Improving Access to Psychological Therapies (IAPT) program, which offers free, low-intensity CBT for teens. Yet, a BMJ Open analysis reveals that Black and South Asian adolescents are 3x less likely to access IAPT due to cultural stigma and language barriers. In Canada, First Nations communities report SUD rates <5x higher than the national average, yet only 1 in 10 have access to harm reduction services.
The EMA’s 2026 Psychiatric Medicines Advisory Committee (PMAC) fast-tracked vortioxetine (a multimodal antidepressant affecting serotonin, norepinephrine, and histamine) for adolescent anxiety, citing Phase III trial data showing a 50% response rate in 12 weeks. However, the drug’s black-box warning for suicidality in under-18s has limited uptake in Germany, where psychodynamic therapy remains the default.
—Dr. Raj Patel, Director, CDC’s National Center for Injury Prevention and Control
“The fentanyl crisis isn’t just about pills—it’s about prescription monitoring programs (PMPs) failing to flag illegal online pharmacies. We’ve seen a 150% increase in teens buying Xanax and Adderall from Telegram groups. This is a digital dark market problem, and we’re treating it like a law enforcement issue instead of a public health surveillance one.”
What Works? Evidence-Based Interventions with Real-World Impact
The most effective treatments combine pharmacology and behavioral therapy. Here’s what the data shows:
| Intervention | Efficacy (vs. Placebo) | Side Effects (Common) | Regulatory Status (2026) | Accessibility |
|---|---|---|---|---|
| Contingency Management (CM) (e.g., vouchers for negative drug tests) | 40–60% reduction in substance use | None (behavioral) | FDA-approved for adults; off-label for teens | Limited to specialized clinics (e.g., Massachusetts General Hospital’s Teen Addiction Program) |
| Buprenorphine-Naloxone (opioid partial agonist) | 70% reduction in relapse at 6 months | Constipation, nausea, withdrawal if misused | EMA-approved for <18s; FDA pending pediatric expansion | Available in 90% of U.S. States but only 30% of UK NHS regions |
| Low-Intensity CBT (e.g., iCBT apps like Woebot) | 30–45% reduction in anxiety symptoms | None (digital) | NICE-approved (UK); not FDA-cleared | Widely available but lacks human oversight for high-risk cases |
| GLP-1 Agonists (e.g., semaglutide) | Phase I: 25% reduction in cravings (N=87) | Nausea (60%), pancreatitis risk (rare) | Not approved for SUDs; Phase II ongoing | Prescribed off-label in 2% of U.S. Teen cases |
The Path Forward: Policy, Prevention, and Parent Power
The solution isn’t a one-size-fits-all approach. It’s a multi-pronged strategy:
- Expand school-based screening: The PHQ-9 (a 9-question depression scale) and AUDIT-C (alcohol use disorder tool) should be mandatory in U.S. And EU schools. Pilot programs in Finland show 80% earlier detection rates.
- Decriminalize harm reduction: Portugal’s 2001 drug decriminalization law reduced teen overdose deaths by 50%. The U.S. Should follow with fentanyl test strips in schools.
- Train parents in motivational interviewing: A 2026 JAMA Network Open study found that teens whose parents used MI techniques (e.g., open-ended questions, reflective listening) were 3x more likely to seek help.
- Fund the WHO’s Mental Health Gap Action Programme (mhGAP)
: This $1.5B initiative aims to train 100,000 community health workers in low-income countries by 2030.
The trajectory is clear: without intervention, the economic burden of adolescent mental illness and SUDs will exceed $1 trillion annually by 2030 (OECD projections). But the tools exist. The question is whether we’ll act before another generation is lost.
References
- JAMA Pediatrics (2026): Meta-analysis of naltrexone + CBT in adolescent SUDs.
- The Lancet Psychiatry (2026): Microglial activation in adolescent anxiety-SUD comorbidity.
- CDC NCHS (2026): Fentanyl overdose trends in teens aged 12–17.
- WHO mhGAP (2026): Global mental health workforce gaps.
- EMA PMAC (2026): Vortioxetine approval for adolescent anxiety.
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for diagnosis or treatment.