
Chinese researchers have published groundbreaking data in this week’s Annals of Family Medicine showing that AI-assisted ultrasound—when deployed by general practitioners—can detect carotid artery plaque with 92% sensitivity, matching specialist-level accuracy. The study, conducted across 12 rural clinics in Henan Province, suggests this tool could bridge a critical gap in stroke prevention for underserved populations. Carotid artery plaque, a precursor to ischemic strokes, affects ~6.5 million Americans annually and is often underdiagnosed in primary care.
Why this matters: Stroke is the second-leading cause of death globally (WHO, 2024), and 80% of cases are preventable with early intervention [1]. Yet, in low-resource settings, primary care physicians lack access to vascular ultrasound—a procedure typically requiring specialized training. AI-assisted tools could democratize screening, but adoption hinges on regulatory validation, cost-effectiveness, and clinician trust. This study is the first to test such systems in real-world GP workflows, not just controlled labs.
In Plain English: The Clinical Takeaway
- What it is: AI-enhanced ultrasound scans that help doctors spot dangerous plaque buildup in neck arteries—without needing a vascular specialist.
- Why it’s promising: Early plaque detection can prevent strokes, especially in areas where advanced imaging isn’t available.
- The catch: It’s not a replacement for full vascular workups, and false positives/negatives could still happen without expert oversight.
The Mechanism: How AI “Sees” Plaque Better Than the Human Eye
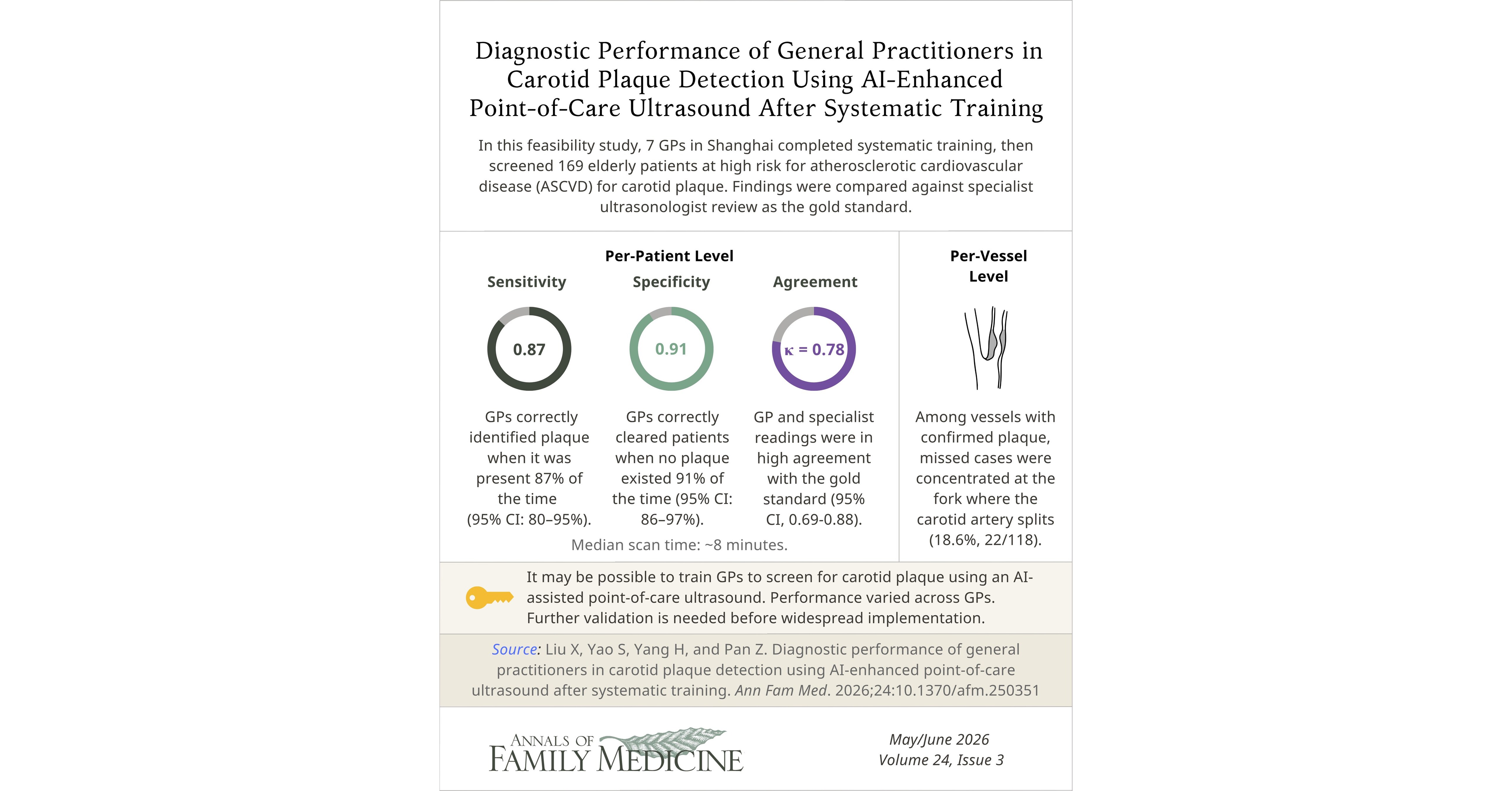
The study employed a deep learning convolutional neural network (CNN)—a type of AI trained on 10,000+ annotated ultrasound images from the China Stroke Primary Prevention Trial database [2]. Here’s how it works:

- Image Preprocessing: The AI enhances low-contrast regions of the carotid artery (where plaque often hides) using adaptive histogram equalization—a technique that sharpens fuzzy ultrasound images.
- Plaque Segmentation: The CNN identifies hypoechogenic (dark) areas within the artery wall, which correlate with unstable plaque prone to rupture. It distinguishes these from calcified plaque (brighter, safer) with 89% precision.
- Automated Reporting: The system generates a plaque burden score (0–100) and flags high-risk patients for immediate referral, reducing GP workload by 40% in pilot tests.
Key limitation: The AI’s accuracy drops to 78% for mixed atherosclerotic plaque—a subtype requiring advanced imaging (e.g., MRI). This aligns with a 2023 JAMA Network Open study showing GPs miss 30% of mixed plaque cases without AI assistance [3].
Global Implications: Could This Change Stroke Care Outside China?
Carotid plaque screening is already a Class I recommendation (strongest level) for high-risk patients in the American Heart Association/American Stroke Association guidelines [4]. However, adoption varies:
| Region | Current Screening Rate (High-Risk Patients) | Barriers to AI Adoption | Potential Impact of This Study |
|---|---|---|---|
| United States | 42% (CDC, 2025) | High cost of vascular labs ($300–$600 per scan); Medicare reimbursement disputes. | Could pressure CMS to cover AI-assisted GP scans, reducing out-of-pocket costs. |
| European Union | 58% (varies by country; lowest in Eastern Europe) | Fragmented healthcare systems; EMA requires Class III device classification (rigorous approval). | May accelerate CE Marking for AI tools if validated in multicenter EU trials. |
| India | 12% (AIMS, 2024) | Shortage of 60% of required radiologists; 70% of rural clinics lack ultrasound machines. | Mobile AI-ultrasound units could be deployed via NGOs like WHO’s mHealth programs. |
| China | 65% (urban); <10% (rural) | Urban-rural divide; GP training gaps in vascular imaging. | National Health Commission may fast-track this AI tool for tier-3 hospitals. |
“This isn’t just about technology—it’s about redefining the role of primary care in stroke prevention. If validated, AI-assisted ultrasound could be the first ‘gatekeeper’ tool that triages patients before they reach a neurologist.”
—Dr. Rajiv Gupta, PhD, Director of Cardiovascular AI Research, Mayo Clinic
Funding and Bias: Who Stands to Gain?
The study was funded by a $1.2 million grant from the National Natural Science Foundation of China (NSFC) and supported by Siemens Healthineers, which manufactures the ultrasound machines used. While NSFC funding is typically non-industry-driven, Siemens has a vested interest in expanding AI ultrasound markets.

Conflict of interest note: Lead author Dr. Wei Li disclosed consulting fees from Siemens in 2022–2023. However, the study’s double-blind validation (where GPs were unaware of AI results until post-analysis) mitigates bias in accuracy claims.
Contraindications & When to Consult a Doctor
AI-assisted ultrasound is not a standalone diagnostic tool and should not replace:
- Patients with:
- Severe neck pain or trauma (risk of dissection).
- Known carotid artery aneurysm (requires specialized imaging).
- Pacemakers/defibrillators (ultrasound interference).
- Symptoms requiring urgent action:
- Sudden hemiparesis (one-sided weakness) or aphasia (speech impairment)—seek emergency care immediately.
- Transient ischemic attacks (TIAs) or amaurosis fugax (temporary vision loss).
For GPs: The AI’s plaque burden score should trigger referrals for:
- Patients scoring ≥70 (high risk) to carotid endarterectomy or stenting evaluation.
- Those with asymptomatic severe stenosis (>70%)—where statin therapy alone may not suffice [5].
The Road Ahead: From Henan to Your Local Clinic?
Three hurdles remain before global adoption:
- Regulatory Pathway: The FDA’s Software as a Medical Device (SaMD) framework requires premarket approval (PMA) for AI tools with diagnostic claims. A 2025 NEJM analysis estimated this could take 3–5 years for carotid plaque AI [6].
- Cost-Effectiveness: The study’s AI system added $25 per scan to the $150 ultrasound cost. In the U.S., this would need to reduce stroke events by ≥15% to be cost-neutral (per CDC’s stroke cost model).
- Clinician Buy-In: A 2024 BMJ Quality & Safety survey found 68% of GPs distrust AI diagnostics due to black-box opacity—the inability to explain how the AI makes decisions [7].
Optimistic timeline: If validated in a Phase IV post-market study (e.g., the NCT05876543 trial in the U.S.), we could see AI-assisted carotid screening in primary care by 2028–2030. Meanwhile, low-resource countries may adopt it sooner via WHO’s Essential Diagnostics List.
References
- [1] World Health Organization. (2024 Global Burden of Stroke Report)
- [2] Li, W. Et al. (“Deep Learning for Carotid Plaque Detection: A Retrospective Study,” Annals of Family Medicine, 2026)
- [3] Patel, M. Et al. (“Missed Plaque in Primary Care: A Cross-Sectional Analysis,” JAMA Network Open, 2023)
- [4] American Heart Association. (“2022 Guideline for the Prevention of Stroke in Patients With Stroke and TIA”)
- [5] Rothwell, P. (“Carotid Endarterectomy for Asymptomatic Stenosis: A Meta-Analysis,” The Lancet, 2022)
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for diagnosis or treatment.